![]() https://doi.org/10.35845/kmuj.2024.23599 ORIGINAL
ARTICLE
https://doi.org/10.35845/kmuj.2024.23599 ORIGINAL
ARTICLE
Nicotine dependency and lung functions of cigarette and
non-cigarette forms of tobacco smokers in Faisalabad, Pakistan
Rehan Anjum![]() 1,
Muhammad Abdullah Babar
1,
Muhammad Abdullah Babar![]() 1,
Shireen Jawed
1,
Shireen Jawed![]() 1,
Farah Amir Ali
1,
Farah Amir Ali![]() 1
1
|
1: Department of Physiology, Aziz Fatimah Medical and Dental College, Faisalabad, Pakistan
Email Contact #: +92-336-3153931
Date Submitted: February 6, 2024 Date Revised: May 20, 2024 Date Accepted: May 27, 2024 |
|
THIS ARTICLE MAY BE CITED AS: Anjum R, Babar MA, Jawed S, Ali FA. Nicotine dependency and lung functions of cigarette and non-cigarette forms of tobacco smokers in Faisalabad, Pakistan. Khyber Med Univ J 2024;16(2):103-9. https://doi.org/10.35845/kmuj.2024.23599 |
ABSTRACT
OBJECTIVES: To compare nicotine dependency and lung functions among cigarette and non-cigarette (e-cigarette & hookah) form of tobacco smokers.
METHODS: This cross-sectional study was conducted from December 2023 and January 2024, at Aziz Fatimah Medical and Dental College, Faisalabad, Pakistan. The study included 100 male tobacco users aged 18 to 60 years, comprising 25 conventional cigarette smokers, 48 e-cigarette users, 25 hookah users, and 2 dual product users. Subjects with known lung diseases (asthma, COPD, tuberculosis), chest deformities affecting lung function, and smokers using nicotine patches or gum for smoking cessation were excluded. Nicotine dependence was assessed using the Fagerström test for nicotine dependence (FTND) and its adapted versions (eFTND) for hookah and e-cigarettes. Lung function parameters, were measured using a digital spirometer.
RESULTS: Mean±SD FTND and eFTND scores for cigarette, e-cigarette, hookah, and dual users were 5.44±1.91, 6.25±2.20, 4.84±1.106 and 5.50± 0.707 respectively (p=0.027). FEV1 of cigarettes, e-cigarettes, hookah, and dual product users were 4.44± 2.69, 4.04±1.56, 3.28±2.21 and 4.72±0.763 respectively (p-value=0.84). FVC for the same groups were 5.86±3.33, 4.35±1.79, 3.7±2.58, and 5.05±0.53 (p=0.012) respectively.FEV1/FVC as followed: cigarettes, 79.44±14.88; e-cigarettes, 94.20±6.5; hookah, 87.39±13.8; dual products, 93.29±5.16 (p-value=0.000). PEF of cigarettes, e-cigarettes, hookah, and dual product users were 7.35±3.71, 8.18 ±2.52, 5.4±3.4, 8.45±0.19 respectively (p-value=0.001).
CONCLUSION: This study reveals significant differences in nicotine dependency and lung function among tobacco-users. E-cigarette users have the highest nicotine dependence but less short-term lung impairment than hookah users. Targeted public health interventions, stricter advertising regulations, and multi-center studies on larger populations are recommended.
KEYWORDS: Vaping (MeSH); Tobacco Products (MeSH); Tobacco (MeSH); Tobacco, Smokeless (MeSH); Waterpipe (MeSH), Electronic Nicotine Delivery Systems (MeSH),E-Cigarette Vapor(MeSH), Tobacco Use Disorder (MeSH), Hookah (Non-MeSH)
INTRODUCTION
Tobacco consumption is one of the major public health problems that impact millions of people globally.1 According to Global Burden of Disease Study 2019, despite a yearly decline of over 1% in age-standardized tobacco smoking exposure from 2010 to 2019, tobacco remains the third leading risk factor for attributable disability adjusted life years(DALYs) among level 2 risks. In 2019, smoking was the second leading risk factor, accounting for 7.9% (7.2 to 8.6) of DALYs.2Despite the Government of Pakistan's efforts to control tobacco use since ratifying the WHO Framework Convention on Tobacco Control (FCTC) in 2004, a nationwide survey indicates that the prevalence of tobacco consumption in Pakistan has increased to 45.5%.1
Tobacco products are available in various forms, such as cigarettes, hookahs, and e-cigarettes (vapes), each containing different amounts of nicotine, a highly addictive substance with numerous health risks, including lung diseases.3E-cigarettes, which deliver nicotine, are becoming increasingly popular among both younger and middle-aged individuals worldwide. This rise in popularity is based on the belief that e-cigarettes have fewer or no harmful effects on health and can assist in quitting cigarette smoking.4,5Nicotine dependence is a significant outcome of any nicotine-containing product, characterized by the psychological and physiological inability to cease its use despite recognizing its harmful effects.6 This dependency can impair lung function by diminishing the quantity and quality of air reaching the lungs, thereby elevating the likelihood of respiratory infections and inflammation, and altering the structure and function of lung tissues.7,8
Lung diseases are significant contributors to mortality and disability in Pakistan, where nicotine usage is widespread among adults and adolescents. Moreover, there exists a considerable economic burden associated with major smoking-related illnesses such as pulmonary, cardiovascular, and cancer conditions, including both medical and non-medical expenses.9 It is estimated that approximately 80% of tobacco consumers worldwide reside in low to middle-income countries, where tobacco-related diseases exacerbate poverty levels.1
The Fagerström Test for Nicotine Dependence (FTND) is a widely employed, validated, and standardized scale for gauging nicotine dependency in cigarette smokers. Recently, researchers have utilized its modified and validated version, eFTND, to assess nicotine dependence in non-cigarette smokers, including e-cigarette and hookah users. The scores from FTND and eFTND categorize subjects into low, moderate, and high nicotine dependency levels for cigarette and non-cigarette smokers, respectively.10,11
This study aimed to assess nicotine dependence and lung function in cigarette and non-cigarette tobacco smokers in Faisalabad city of Pakistan. It provides critical insights into the impact of various forms of tobacco smoking on lung health and nicotine dependency, highlighting the addictive nature of these smoking devices. By offering new data from Pakistan, this study contributes to the existing literature on the controversial issues of whether e-cigarettes serve as a cessation pathway for cigarette smoking or as a gateway to initiating smoking again due to e-cigarette-induced nicotine dependency. The findings will also inform government and policymakers, aiding them in making decisions to ban these hazardous devices to reduce the burden of nicotine-related diseases and deaths.
METHODS
This cross sectional study was conducted at Aziz Fatimah Medical and Dental College, Faisalabad, Pakistan, from December 2023 to January 2024 after getting ethical approval from the Institutional Ethical Committee (IEC) with reference #IEC/253-23. The sample size was calculated by power and sample size (PS) software using mean α value 0.05, power 80%, CI 95% mean difference, and SD of nicotine dependency scores of 1.2 and 2.1 respectively taken from a previous study.12 Sample size calculated was 98 subjects, additionally, we enrolled two participants to make a sample size of 100 participants.
The study included male subjects aged 18 to 60, who smoked tobacco daily in the form of conventional cigarettes, nicotine-based e-cigarettes (vape), conventional hookah, or used dual products for at least six months. Those using e-cigarettes or conventional hookah were classified as non-cigarette tobacco users. Participants were recruited using convenience sampling technique. Individuals with known lung diseases (asthma, COPD, tuberculosis), chest deformities affecting lung function (such as pectus excavatum, pectus carinatum), female subjects, and smokers using smoking cessation therapies like nicotine patches or gum were excluded from the study.
Informed consent was obtained from each participant, and pertinent smoking details, such as smoking status (current or ex-smoker), age at smoking initiation, average smoking duration, daily cigarette consumption, smoking type, pack-years, and motives for tobacco product use, were documented on a structured form.
FTND and its modified version, eFTND, were utilized to assess nicotine dependency in cigarette and non-cigarette smokers, respectively. 10,11 FTND comprises six items that evaluate cigarette consumption, compulsion to use, and dependence. In scoring the FTND, yes/no items are scored from 0 and 1, and multiple-choice items are scored from 0 to 3. The items are summed to yield a total score of 0 to 10. The modified eFTND is also a valid and reliable instrument with a Cranach α value of 0.725. It has scores such as the original scale, that is, from 0 to 10 with equivalent six questions. The principal change was only the change in terminology and cigarettes were replaced by e-cigarettes or hookahs.11 The FTND and e-FTND scores of 1–3, 4–6, and 7–10 categorized the smokers as low, medium, and high nicotine dependence categories respectively.11
Pulmonary function test variables including Forced Vital Capacity (FVC), Forced Expiratory Volume in the 1st second (FEV1), FEV1/FVC ratio, and the Peak Expiratory Flow Rate (PEF), were determined by a digital spirometer (Bionet Cardiotouch 3000) according to the acceptability standard specified by the American Thoracic Society/European Respiratory Society Task Force (AST/ERS).13 Spirometry was performed with subjects in the sitting position and using nose clips. Sterile mouthpieces were used to prevent any cross-infections for each participant. Three maneuvers were performed for each subject and the highest value was recorded for each parameter by analyzing the obtained spirogram. Nicotine dependency scores and lung function parameters were compared among the cigarette and non-cigarette forms of tobacco smokers.
Data was analyzed by SPSS 26. Mean and standard deviations were calculated for continuous variables. Frequencies and percentages were determined for categorical variables. ANOVA was employed to compare mean FTND scores and spirometric parameters, followed by post hoc tests for multiple comparisons. A significance level of P ≤ 0.05 was adopted.
RESULTS
This study consisted of 100 male participants with an age range of 33.02±12.40 years. Out of the 100 participants, 48 (48%) participants reported consumption of nicotine by e-cigarette use exclusively, and 25 (25%) reported smoking conventional cigarettes. Another 25 (25%) reported using hookah whereas; only 2 (2%) participants reported the use of dual products.
Mean± SD of pack years of exclusive cigarette users was12.36±10.44 years and of dual product users who used cigarette as well as vape was 4.125±4.77 years.
Results revealed that 76% of cigarette smokers, 50% of e-cigarette users and 48% of hookah users smoked due to peer pressure. While 12% of cigarette smokers, 20% e-cigarette users and 32% of Hookah users using these products as a symbol of status (Table I).
Table 1: Distribution of Reasons for Using Cigarettes and Non-Cigarette Forms of Tobacco Smoking (n= 100)
|
B |
Cigarette smokers (n=25) |
E-Cigarette users (n=48) |
Hookah users (n=25) |
Dual product users(n=2) |
|
Frequency (%) |
Frequency (%) |
Frequency (%) |
Frequency (%) |
|
|
Peer Pressure |
19 (76) |
24 (50) |
12 (48) |
0 (0) |
|
Status symbol |
3 (12) |
20 (41.7) |
8 (32) |
2 (100) |
|
Commonly used by Family members |
2 (8) |
2 (4.15) |
5 (20) |
0 (0) |
|
Without reason |
1 (4) |
2 (4.15) |
0 (0) |
0 (0) |
|
|
Among the cigarette smokers, the majority (64%) of the respondents scored between 5 and 7 (moderate dependence), 20% scored between 3 to 4 (low to moderate), and only 12% scored >8 and fell in the category of high dependency. In comparison to this 54% of e-cigarette users scored between 5 and 7 and 29.2% scored >8 and fell in the moderate and high dependency respectively. Among the hookah users the majority (52%) scored between 2 and 3 and fell in the low to moderate category of nicotine dependency and 48% scored 5 to 7 and were in moderate dependency however, not a single hookah user showed high nicotine dependence (Table II).
Table II: Nicotine dependency cigarettes and non-cigarettes form of tobacco users (n=100)
|
Nicotine Dependency |
Cigarettes smoker (n = 25) |
E- Cigarettes users (n= 48) |
Hookah users (n=25) |
Dual product users (n =2) |
|
Low dependency (score 1-2) |
1(4) |
4(8.3) |
00 |
00 |
|
Low to moderate dependency (score 3-4) |
5(20) |
4(8.3) |
00 |
2(100) |
|
Moderate dependency (score 5-7) |
16(64) |
26(54.0) |
13(52) |
00 |
|
High dependency (score >8) |
3(12) |
14(29.2) |
12(48) |
00 |
The mean±SD FTND & eFTND scores of cigarette and non-cigarette forms of tobacco consumers are presented in Figure 1. We noticed significantly higher mean scores for nicotine dependency among the e-cigarette users and lower scores were found among hookah users with p-value=0.027 (Figure 1).
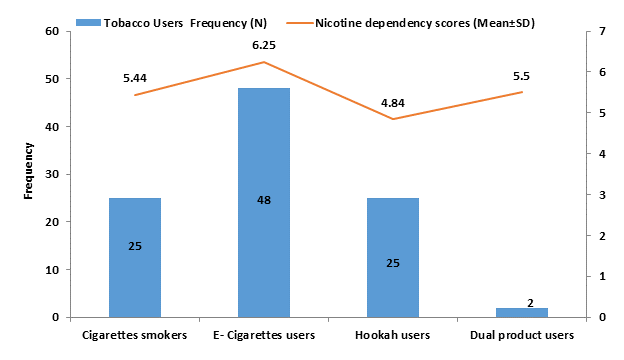
Figure 1: Nicotine dependency scores of cigarettes and non-cigarette forms of tobacco smokers (n=100)
We noticed lower FVC levels in hookah smokers followed by e-cigarette users, whereas FEV1/FVC ratios were lowest among subjects smoking cigarettes. Mean FVC and FEV1/FVC were significantly different among the study groups with p values = 0.012& 0.000 respectively (Table III). Post hoc multiple comparisons revealed significant differences in the mean FVC between cigarette and hookah users (p= 0.007). The FVC/FEV1 ratio of e-cigarette smokers was significantly different from that of cigarette smokers (p = 0.000) and hookah users (p = 0.010). The mean PEF values for hookah users were significantly different from those of cigarette smokers (p = 0.046) and e-cigarette users (p = 0.000).
FEV1 levels were lower in hookah users compared to other groups, but the mean differences were not statistically significant (P = 0.84). PEF was highest in dual product users (e-cigarettes and cigarettes) and lowest among hookah users. The mean PEF values differed significantly among the study groups (p = 0.001) [Table III]. Post hoc multiple comparisons revealed significant differences in PEF between e-cigarette and hookah users (p = 0.037).
Table III: Comparison of lung function parameters among study groups (n=100)
|
Tobacco smokers |
Force expiratory volume in first second (FEV1) |
Forced volume capacity (FVC) |
Force expiratory volume in first second/ Forced volume capacity (FEV1/FVC) |
Peak expiratory flow (PEF) |
|
Cigarettes |
4.44± 2.69 |
5.86 ±3.33 |
79.44±14.88 |
7.35 ± 3.71 |
|
E-cigarettes |
4.04±1.56 |
4.35 ±1.79 |
94.20 ±6.53 |
8.18 ±2.52 |
|
Hookah |
3.28± 2.21 |
3.7±2.58 |
87.39±13.8 |
5.4 ±3.4 |
|
Dual products |
4.72± 0.763 |
5.05 ±0.53 |
93.29 ±5.16 |
8.45 ±0.19 |
|
P-values |
0.84 |
0.012* |
0.000* |
0.001* |
P-value≤ 0.05 considered significant.
Post hoc analysis: P values are significant among cigarette and hookah for FVC (p-value 0.007)
P value are significant e-cigarette vs cigarette (p value 0.000) and e-cigarette vs hookah (p value 0.010 value) for FEV1/FVC
P values are significant among cigarette and hookah for PEF (p-value 0.037)
Table IV presents a comparison of age and duration of tobacco use among the study groups. Hookah users were older and had a longer duration of tobacco use compared to cigarette and e-cigarette smokers. Statistically significant differences were observed in both age (p = 0.000) and duration of use (p = 0.000) among the study groups.
Table IV: Comparison of age and duration of the Cigarette and Non-Cigarette Forms of Tobacco Smokers
|
|
Cigarettes smoker (N = 25) |
E- Cigarettes users (N= 48) |
Hookah users (N=25) |
Dual product users (N =2) |
p-value |
|
Age (years)
|
36.92±11.416 |
27.95±7.754 |
46.48±8.21 |
22.5±22.50 |
0.000* |
|
Duration(years)
|
11.96±8.81 |
4.062±954 |
12.32±5.76 |
4.00±1.41 |
0.000* |
Data is presented as mean and standard deviation
DISCUSSION
Tobacco consumption in the form of e-cigarettes as an alternative to conventional cigarettes has seen a surge in popularity over recent years; however, this growing popularity has generated a debate in public health sectors concerning its safety and effectiveness as a potential smoking cessation tool.
In the current study, the majority of the population consumed tobacco in the form of cigarettes, e-cigarettes, and hookah due to peer pressure, whereas participants who used dual products reported using these products as a symbol of status. In contrast to our study, the majority of participants (66.7%) in the Sreeramareddy CT study believed that e-cigarette was a safer alternative to conventional cigarettes. Furthermore, the main reason for using e-cigarettes was to avoid and quit cigarette smoking in the aforementioned study.12
In the current study, a higher dependence was noticed among exclusively e-cigarette users and they have comparatively higher eFTND scores than cigarette, hookah, and dual product users. The majority of conventional cigarette smokers had moderate to high dependency, whereas hookah users had low to moderate nicotine dependency. Our findings suggested that e-cigarettes can act as a gateway for cigarette smoking due to their higher addictive potential. In contrast to our results, previous studies conducted in Karachi, Pakistan by Zaidi AB.5 and in the USA by Liu G, et al.,. found lower nicotine dependency scores among e-cigarette users than cigarette smokers and dual product users. Our results concerning the comparison of e-cigarettes and cigarettes are in line with Jankowski M, et al., who reported two times higher significant nicotine dependence levels estimated by FTND among e-cigarette users compared to cigarette smokers.15
Concerning the comparison of e-cigarettes and dual products our results are not comparable with the study conducted in Malaysia by Sreeramareddy et al.12 who reported that exclusively e-cigarette use had a lower dependence and significantly lower eFTND scores than those who were using dual products (3.0±1.6 vs. 5.3±2.6). This aforementioned study suggested that dual product users would be consuming a higher amount of nicotine that was present in both of the tobacco products and that’s why they have more nicotine dependency.12 Jankowski M, et al.,15 found an interesting finding and noticed a higher nicotine dependence level in the group of dual users when using an e-cigarette compared to conventional cigarette smoking. These findings reflect that dual users have a higher dependency because of e-cigarettes. Furthermore, Jankowski M, et al., suggested that e-cigarette users may be at higher risk of addiction due to high nicotine dependency compared to cigarette smokers.15 Conflicting results have been documented by previous studies concerning the addictive nature of e-cigarettes, which are documented to be less addictive than conventional cigarettes by some researchers, however, some suggest that e-cigarettes may have a higher addictive potential than cigarette smoking.14,15
In the current study, we found the lowest FTND scores in hookah users as compared to cigarette and e-cigarette users. Most hookah users were in the category of low to moderate nicotine dependency and not even a single user had high nicotine dependency. Our findings suggested that it is a less addictive form of tobacco consumption as compared to other tobacco products. These results are supported by a previous Pakistani study conducted in Sargodha Pakistan which reported comparatively lower nicotine dependency, and FTND score among participants who smoked hookah exclusively as compared to cigarette smokers (4.7±2.1 vs. 5.4±2.2).
In current study hookah users were older as compared to cigarette smokers and were used hookah for long duration as compared to cigarette and e -cigarette smokers. Our findings concerning age and duration of tobacco consumption is in agreement with the Pakistani study conducted by Dogar O, et al., hookah users of their study were older as compared to cigarette smokers and used hookah for a longer duration. Moreover, majority of the hookah users in the aforementioned study had low to moderate nicotine dependency and few had high nicotine dependency, even using it for a longer duration.16
Current study reveals that hookah and e-cigarette users have lower FVC and FEV1 values as compared to conventional cigarette smokers and dual product users. TheFEV1/FVC ratio was significantly reduced in cigarette smokers. The reported findings concerning FEV1 are also in agreement with Darabseh MZ, et al.,17 who found lower FEV1 among e-cigarette and cigarette smokers as compared to control and did not find significant differences among e-cigarette and cigarette smokers. In contrast to our study, this aforementioned study documented declined FEV1/FVC in both e-cigarette and cigarette smokers.17 Polosa et al. did not find decrements in the spirometric indices, FEV1, FVC, and FEV1/FVC ratio among e-cigarette smokers and no significant difference was found between e-cigarette users and control subjects.18 The reporting of Polosa R, et al.,concerning FVC, and FEV1/FVC ratio are in line with our results. The discrepancy between reports of these previous and current studies might be due to the duration of e-cigarette use, frequency/intensity of e-cigarette smoking, or nicotine concentration in the liquid used for e-cigarettes. It is evident from previous studies that inhaled nicotine has adverse pulmonary effects.19In the current study we also found significantly lower PEF in hookah users as compared to other groups. Current results are incongruent with the results of the Koubaa A, et al., study which also found the lowest PEF values among hookah smokers as compared to cigarette smokers and non-smokers (hookah smokers =93.1±7.9 vs. cigarette smokers =95.5±4.5 vs. non-smokers=100.5±5.8).20 In contrast to the current study, the PEF rate remained in the green zone in 90% of the study population in the study conducted by Sultanov and colleagues.21
However, we found slight variations in spirometry parameters among the study groups but these values were within normal physiological limits may be because we also enrolled the cigarette and e-cigarette users with a short duration of at least 6 months. Our results are justified by the non-randomized repeated-measures controlled study by Flouris et al. who concluded that short-term use of e-cigarettes generates minimal changes in spirometric parameters without any significant clinical impact, but has a similar nicotinergic impact to conventional cigarettes.22 Another clinical trial conducted in the UK distinguished the effects of short-term, 1-month, 3-month, and 24-month e-cigarette inhalation on lung function. This study found a slight decline in baseline FEV1, FVC, FEV1/FVC, and PEF at the 3rd and then 24th-month follow-up, which was not clinically relevant.23 These researches collectively reflect that the short-term usage of tobacco especially in the form of e-cigarettes may not have a significant effect on lung function, however, if used for a longer duration may adversely harm lung function, so long-term effects need to be studied by longitudinal studies or clinical trials. e-cigarettes are harmful and addictive. Further education and legislation are needed to prevent and stop its use.
CONCLUSION
This study reveals significant differences in nicotine dependency and lung function among users of various tobacco products. e-cigarette users exhibit the highest nicotine dependence, followed by conventional cigarette smokers, dual product users, and hookah users. Regarding negative impact on respiratory health, E-cigarette users show relatively less effects on lung function (highest FEV1/FVC ratio) compared to hookah users. Although short-term tobacco inhalation does not significantly impact lung function, the long-term effects, particularly of e-cigarettes, require further investigation. The recent rise in e-cigarette marketing, promoted as a less harmful alternative, has increased its consumption among the younger generation. These findings highlight the need for targeted public health interventions, multi-center studies on larger populations, and stricter regulations on e-cigarette advertising to better understand and mitigate the long-term implications on lung health.
REFERENCES
1. Basit A, Bin Younus B, Waris N, Fawwad A. Prevalence of tobacco use in urban and rural areas of Pakistan; A sub-study from second national diabetes survey of Pakistan (NDSP) 2016-2017. Pakistan J Med Sci 2020;36(4):808-15. https://doi.org/10.12669/pjms.36.4.1705
2. GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020 396(10258):1223-1249. https://doi.org/10.1016/S0140-6736(20)30752-2
3. James PB, Bah AJ, Kabba JA, Kassim SA, Dalinjong PA. Prevalence and correlates of current tobacco use and non-user susceptibility to using tobacco products among school-going adolescents in 22 African countries: a secondary analysis of the 2013-2018 global youth tobacco surveys. Arch Public Heal 2022;80(1):1-15. https://doi.org/10.1186/s13690-022-00881-8
4. Banks E, Yazidjoglou A, Brown S, Nguyen M, Martin M, Beckwith K, et al. Electronic cigarettes and health outcomes: umbrella and systematic review of the global evidence. Med J Aust 2023;218(6):267-75. https://doi.org/10.5694/mja2.51890
5. Zaidi AB, Shaikh S. Nicotine dependence and intention to quit among electronic, conventional and dual cigarette users in Karachi. J Pak Med Assoc 2022;72(9):1766-70. https://doi.org/10.47391/jpma.4188
6. Zuckerman G, Kamke K, Sabado-Liwag M, Pérez-Stable EJ, El-Toukhy S. Noncigarette tobacco product use among smoking-susceptible and nonsusceptible adolescent never smokers, 2009-2021. J Adolesc Heal 2024;74(3):466-78. https://doi.org/10.1016/j.jadohealth.2023.09.021
7. Lazreg NB, Kchaou K, Guezguez F, Barkous B, Khamsa SB. Is nicotine dependence associated with lung function, physical capacity and sleep quality? Eur Respir J 2023;62:PA3317; https://doi.org/10.1183/13993003.congress-2023.PA3317
8. Carroll BJ, Kim M, Hemyari A, Thakrar P, Kump TE, Wade T, et al. Impaired lung function following e-cigarette or vaping product use associated lung injury in the first cohort of hospitalized adolescents. Pediatr Pulmonol 2020;55(7):1712-8. https://doi.org/10.1002/ppul.24787
9. Nayab D, Memon JA, Siddique O, Nasir M, Memon JA, Siddique O. the economic cost of tobacco-induced diseases in Pakistan [Internet]. 2021. Available from URL: https://tobacconomics.org/files/research/677/the-economic-cost-of-tobacco-induced-diseases.pdf
10. Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. the fagerström test for nicotine dependence: a revision of the fagerstrom tolerance questionnaire. Br J Addict 1991;86(9):1119-27. https://doi.org/10.1111/j.1360-0443.1991.tb01879.x
11. Rahman AU, Mohamed MHN, Jamshed S, Mahmood S, Muhammad AIB. The development and assessment of modified fagerstrom test for nicotine dependence scale among malaysian single electronic cigarette users. J Pharm Bioallied Sci 2020;12(suppl 2):S671-5. https://doi.org/10.4103/jpbs.jpbs_245_19
12. Sreeramareddy CT, Shroff SM, Gunjal S. Nicotine dependence and associated factors among persons who use electronic e-cigarettes in Malaysia - an online survey. Subst Abus Treat Prev Policy 2023;18(1):1-11. https://doi.org/10.1186/s13011-023-00558-7
13. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J 2005;26(2):319-38. https://doi.org/10.1183/09031936.05.00034805
14. Liu G, Wasserman E, Kong L, Jonathan F. Comparison of nicotine dependence among exclusive e_cigarette and cigarette users in the PATH study comparison of nicotine dependence among exclusive e_cigarette and cigarette users in the PATH study. Prev Med 2017;104:86-91. https://doi.org/10.1016%2Fj.ypmed.2017.04.001
15. Jankowski M, Krzystanek M, Zejda JE, Majek P, Lubanski J, Lawson JA, et al. E-cigarettes are more addictive than traditional cigarettes—a study in highly educated young people. Int J Environ Res Public Health 2019;16(13):4-13. https://doi.org/10.3390%2Fijerph16132279
16. Dogar O, Jawad M, Shah SK, Newell JN, Kanaan M, Khan MA, et al. Effect of cessation interventions on hookah smoking: Post-Hoc analysis of a cluster-randomized controlled trial. Nicotine Tob Res 2014;16(6):682-8. https://doi.org/10.1093/ntr/ntt211
17. Darabseh MZ, Selfe J, Morse CI, Degens H. Impact of vaping and smoking on maximum respiratory pressures and respiratory function. Int J Adolesc Youth 2021;26(1):421-31. https://doi.org/10.1080/02673843.2021.1976235
18. Polosa R, Cibella F, Caponnetto P, Maglia M, Prosperini U, Russo C, et al. Health impact of E-cigarettes: a prospective 3.5-year study of regular daily users who have never smoked. Sci Rep 2017;7(1):1-9. https://doi.org/10.1038/s41598-017-14043-2
19. Antoniewicz L, Brynedal A, Hedman L, Lundbäck M, Bosson JA. Acute effects of electronic cigarette inhalation on the vasculature and the conducting airways. Cardiovasc Toxicol 2019;19(5):441-50. https://doi.org/10.1007/s12012-019-09516-x
20. Koubaa A, Triki M, Trabelsi H, Masmoudi L, Zeghal haled N, Sahnoun Z. Lung function profiles and aerobic capacity of adult cigarette and hookah smokers after 12 weeks intermittent training. Libyan J Med 2015;10(1):26680. https://doi.org/10.3402/ljm.v10.26680
21. Sultanov S, Fatima T, Sultanova S, Homova N, Rafkat F. Influence of smoking of hookah on some indicators of respiratory system in girls of childbearing age. Eur Respir J 2019;54:PA4478. https://doi.org/10.1183/13993003.congress-2019.PA4478
22. Flouris AD, Chorti MS, Poulianiti KP, Jamurtas AZ, Kostikas K, Tzatzarakis MN, et al. Acute impact of active and passive electronic cigarette smoking on serum cotinine and lung function. Inhal Toxicol 2013;25(2):91-101. https://doi.org/10.3109/08958378.2012.758197
23. Walele T, Bush J, Koch A, Savioz R, Martin C, O’Connell G. Evaluation of the safety profile of an electronic vapour product used for two years by smokers in a real-life setting. Regul Toxicol Pharmacol 2018;92:226-38. https://doi.org/10.1016/j.yrtph.2017.12.010
|
CONFLICT OF INTEREST Authors declared no conflict of interest, whether financial or otherwise, that could influence the integrity, objectivity, or validity of their research work. GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |