![]() https://doi.org/10.35845/kmuj.2024.23452 ORIGINAL
ARTICLE
https://doi.org/10.35845/kmuj.2024.23452 ORIGINAL
ARTICLE
Risk factors for diabetes mellitus among caregivers of dialysis-dependent patients: results from a case-control study in Pakistan
SumairaNasim![]() 1,2,
Nicola
Mary Lowe
1,2,
Nicola
Mary Lowe ![]() 1,
Victoria Hall Moran
1,
Victoria Hall Moran![]() 1,
Stephanie Dillon
1,
Stephanie Dillon![]() 1,
Sidra Zaheer 2
1,
Sidra Zaheer 2
|
1: UCLan Research Centre for Global Development, University of Central Lancashire, Preston, PR1 2HE “UK” 2: School of Public Health, Dow University of Health Sciences, Karachi, Pakistan
Email
Contact #: +92-335-2618247
Date Submitted: August19, 2023 Date Revised: June 13, 2024 Date Accepted: June 19, 2024 |
|
THIS ARTICLE MAY BE CITED AS: Nasim S, Lowe NM, Moran VH, Dillon S, Zaheer S. Risk factors for diabetes mellitus among caregivers of dialysis-dependent patients: results from a case-control study in Pakistan. Khyber Med Univ J 2024;16(2):151-8. https://doi.org/10.35845/kmuj.2024.23452 |
ABSTRACT
OBJECTIVES: To analyze the effect of the caregiver role on the diet intake, physical activity and future risk of developing diabetes mellitus (DM) in adult female carers of patients with long-term illness in Pakistan.
METHODS: This hospital-based case control study was conducted between October 2017 and March 2018 at three dialysis centers located in Rawalpindi, Pakistan. The cases included female caregivers who had been looking after patients with long-term chronic kidney disease for at least 6 months. The comparison group consisted of female caregivers accompanying patients with short-term conditions lasting one month or less. Data on socio-demographic factors, anthropometry, diet, and physical activity were collected. Random measurements of blood glucose, triglycerides, and cholesterol levels were taken. Additionally, the Women's Diet Diversity Score (WDDS) and Finnish Diabetes Risk Score (FDRS) were calculated.
RESULTS: Cases (n=124) compared to controls (n=128) showed higher diabetes risk score (2.51±0.90 vs. 2.22±1.01, p=0.048) and similar WDDS. Both groups exhibited a high prevalence of overweight (BMI >29 kg/m²) and limited fruit intake. Despite similar diet diversity, caregivers reported increased physical activity and altered household responsibilities. More than half of all participants were overweight (BMI >29kg/m2). The mean WDDS of cases and controls were 4.77±1.51 and 4.90±1.62, respectively.
CONCLUSION: Our study shows that overweight and poor diet diversity was prevalent in both groups. The overall risk of chronic disease was low in both groups, however caregivers of patients with long-term illness had higher risk scores for DM than controls.
KEYWORDS: Dialysis (MeSH); Haemodialysis (Non-MeSH), Renal Dialysis (MeSH); Kidney Diseases (MeSH); Renal Insufficiency, Chronic (MeSH); Diabetes Mellitus (MeSH); Caregivers (MeSH); Diet (MeSH);Physical Activity (MeSH); Exercise (MeSH).
INTRODUCTION
Caregiver is “a person who gives significant amounts of help over long periods of time to a relative, friend or neighbor who is ill or disabled”.1 Caregivers typically perform their duties without formal training and often for an unspecified duration. Despite this, they play a vital role in addressing the shortage of human resource in within the healthcare system.2 However, caregivers may encounter economic challenges, social isolation, and health issues due to their care giving responsibilities.3 Research has investigated how caregiving can impact dietary habits and physical activity, potentially increasing the risk of chronic diseases.4-7
In Pakistan, research has investigated the mental health impacts of caregiving.8,9 For instance, a study explored the beliefs and perceptions of parents caring for children with Autism Spectrum Disorder (ASD) through in-depth interviews. While many parents viewed care giving as a noble responsibility, they highlighted challenges such as lack of respite and awareness about ASD, which could contribute to caregiver burden.8However, there remains limited data concerning the physical health implications for caregivers.
Chronic Kidney Disease (CKD) represents a persistent and irreversible public health concern in Pakistan, affecting over 10 million individuals, with hem dialysis (HD) being the standard treatment.10 A cross-sectional study in Karachi indicated that 52% of CKD patients opt for HD as their preferred management strategy.11 The care giving burden can be especially significant for those caring for patients undergoing long-term HD, as it involves frequent and lengthy hospital visits, typically three to four times per week.12
In Pakistani culture, most caregivers are women who balance multiple gender-specific responsibilities within their families and for the patients. Female caregivers are emotionally invested in the health and well-being of care recipients, but they often encounter time constraints, financial burdens, and limited health literacy, which elevate their risk of chronic diseases. Unlike in high-income countries, the Pakistan government and healthcare system lack adequate support systems to provide caregivers with respite.13
Given the scarcity of information on the impaired lifestyle of female caregivers, this study was planned to explore the diet, physical activity, and health status of female caregivers. Additionally, it aimed to compare the risk of developing chronic diseases between female caregivers of patients with long-term illnesses such as CKD and a control group of women attending hospitals with acute care patients, in an urban setting in Pakistan.
METHODS
A comparative cross-sectional study design was employed, where Group A consisted of caregivers of patients with a long-term condition (CKD), referred to as "cases". These were compared with Group B, comprising caregivers of patients attending the same hospital with an acute condition, referred to as "controls".
Using convenience sampling, data were collected between October 2017 and March 2018 from three dialysis centers (Dialysis Unit of the Pakistan Kidney Patient Association, Rawalpindi, Bahira International Hospital, and Fauji Foundation Hospital) in Rawalpindi, Pakistan.
The inclusion criteria for cases included adult females caring for a hemodialysis patient unpaid for at least six months. The control group comprised adult females accompanying family members with acute illness for one month or less, selected from the same hospital to ensure socioeconomic similarity. Pregnant and lactating women were excluded from both groups. Given the chronic nature of CKD, caregivers of hemodialysis patients were expected to experience greater burden compared to those caring for patients with acute illness.
The sample size was determined using an online sample size calculator (Openepi) based on the proportion of participants with high total cholesterol levels observed in a study: 54.8% in Group A (cases) and 24.1% in Group B (controls). 14 With 80% power and a 95% confidence level, a minimum sample size of 80 participants was calculated, requiring 40 participants in each group.
Ethics approval for the study protocol was granted by the University of Central Lancashire, ethics committee (STEMH 693), Preston, UK, on August 23, 2017.
Prior to data collection, a pilot study was conducted to assess the suitability of selected tools and research strategies. Consent to access participants was obtained from the administration departments of the participating hospitals.Dueto cultural considerations, data collection took place in a waiting room near the HD ward, ensuring females could comfortably provide anthropometric measurements in light clothing and have the option to remove their veils for privacy. The first author, a registered dietitian in Pakistan, collected the data in the waiting room designated for caregivers.
Using interviewer-administered questionnaire information was gathered regarding age, marital status, years of education, living arrangement and household income. The data were also collected regarding the care-recipients including years of dialysis, co-morbidities and frequency of HD.
Weight, height, waist circumference, and hip circumference were measured following the WHO protocol.14 Weight was measured using an electronic weighing scale with participants in light clothing and without shoes. Height was measured using a stadiometer after participants removed footwear and any hair accessories affecting height. Body Mass Index (BMI) was calculated (kg/m²) and categorized to assess the risk of chronic diseases in the South Asian population.15
Biochemical tests were performed immediately after gathering study information through a questionnaire. Tests included measuring total blood cholesterol, blood triglycerides, and blood glucose using capillary blood samples from a finger and a PRIMA test meter (Antonio Monti 7 CH - 6828 Balerna Switzerland). All biochemical tests were provided free of charge to study participants.
Information regarding participants' current and past medical history, including gestational diabetes mellitus, current blood pressure (BP) or the intake of medicine for chronic illness was collected.
Dietary intake was evaluated through a combination of methods including a 24-hour recall interview and completion of a short Food Frequency Questionnaire (FFQ). The 24-hour recall utilized a multiple pass technique to ensure comprehensive data collection on food items consumed. Additionally, open-ended questions explored participants' diet history and the influence of care giving responsibilities on dietary patterns. The FFQ encompassed all major food groups such as fruits, vegetables, dairy, meat (or alternatives like lentils), oils and spreads, and discretionary items (e.g., bakery products). Participants reported the frequency of consumption for each group ranging from never to four or more times per day.
The following two additional short questions were asked:
· Do you think your daily routine has changed since becoming a caregiver? Yes/No If yes, please explain.
· Do you think that your diet intake has changed since becoming a caregiver? Yes/No If yes, please explain.
Participants' physical activity levels were assessed by inquiring about their daily household activities, supplemented by a specific question: "Do you typically engage in at least 30 minutes of physical activity daily at work and/or during leisure time, including normal daily activities?"
The dietary data obtained from the 24-hour diet recall was used to compute the Women's Dietary Diversity Score (WDDS). Participants consuming fewer than five food groups were categorized as having poor diet diversity (WDDS < 5).16
The risk of developing chronic disease was assessed using blood biochemical parameters (random blood glucose, triglycerides, and cholesterol) along with the Finnish Diabetes Risk Score (FDRS). This tool includes eight questions covering both modifiable and non-modifiable risk factors for Type 2 diabetes mellitus (T2DM), such as age, anthropometrics (BMI and waist circumference), physical activity, fruit and vegetable intake, medical history, and use of medications for hypertension. Each question is scored based on its associated risk for T2DM, resulting in a total score ranging from 0 to 26 points (0=no risk, 26=maximum risk). Scores below seven indicate low risk, 7 to 11 suggest slightly elevated risk (approximately 1 in 25 individuals will develop diabetes), 12-14 indicate moderate risk (approximately 1 in 6 individuals will develop diabetes), 15 to 20 indicate high risk (approximately 1 in 3 individuals will develop diabetes), and scores above 20 indicate very high risk (approximately 1 in 2 individuals will develop diabetes).18
Data were analyzed using SPSS version 27.0 (SPSS Inc., Chicago, IL, USA) and STATA version 14. Continuous variables such as FDRS, WDDS, and anthropometric measures were presented as Mean±SD, while categorical variables reflecting participants' socio-demographic characteristics were presented as frequencies and percentages. Independent t-tests were used to compare mean differences between cases and controls for quantitative measures, while Pearson’s chi-square or Fisher’s exact tests were employed to assess associations between cases and controls for categorical variables.
Further stratified analyses were conducted to explore the relationship of FDRS with BMI, WDDS, and biochemical markers. Independent t-tests and one-way ANOVA were performed to compare mean FDRS scores between cases and controls separately for WDDS, BMI, and clinical/biochemical markers. A significance level of p ≤0.05 was considered statistically significant.
RESULTS
A total of 124 cases (49.20%) and 128 control participants (50.79%) were initially recruited. No questionnaires were excluded, but there were missing data for various variables due to participants refusing anthropometric measurements or blood tests. As a result, FDRS calculations were feasible for 78 (63%) cases and 91 (71%) control participants.
Table 1 presents the socio-demographic characteristics of each study participant. There were statistically significant differences between cases and controls in terms of employment status; specifically, 101 (81.5%) cases were unemployed compared to 72 (56.2%) controls (p <0.01).
Table I: Comparison of sociodemographic characteristics between cases and controls (n=252)
|
Cases |
Controls |
Test statistic
|
p-value |
||
|
N (%) |
N (%) |
||||
|
Family structure |
Nuclear |
50 (40.3%) |
66 (51.6%) |
3.203 |
0.074 |
|
Joined |
74 (59.7%) |
62 (48.4%) |
|||
|
Years of Education |
No Education |
20 (16.1%) |
19 (14.8%) |
25.954 |
<0.001 |
|
Till five years |
9 (7.3%) |
13 (10.2%) |
|||
|
Till ten years |
29 (23.4%) |
28 (21.9%) |
|||
|
Till twelve years |
33 (26.6%) |
61 (47.7%) |
|||
|
> Fourteen years |
33 (26.6%) |
7 (5.5%) |
|||
|
Residence |
Rawalpindi |
93 (75.0%) |
104 (81.2%) |
1.442 |
0.231 |
|
Other cities |
31 (25.0%) |
24 (18.8%) |
|||
|
Occupation |
Employed |
23 (18.5%) |
56 (43.8%) |
18.587 |
<0.001 |
|
Unemployed |
101 (81.5%) |
72 (56.2%) |
|||
|
Marital status |
Single |
27 (22.0%) |
25 (19.5%) |
0.224 |
0.636 |
|
Married |
96 (78.0%) |
103 (80.5%) |
|||
|
Income category (PKR)
|
<30,000 |
38 (30.6%) |
33 (25.8%) |
22.585 |
<0.001 |
|
30001-50,000 |
24 (19.4%) |
32 (25.0%) |
|||
|
50,001-70,000 |
10 (8.1%) |
13 (10.2%) |
|||
|
More than 70,000 |
14 (11.3%) |
36 (28.1%) |
|||
|
Refused or Not known |
38 (30.6%) |
14 (10.9%) |
|||
p-value calculated using Fisher’s exact test/Chi-square analysis; PKR: Pakistani rupees
Additionally, a higher proportion of cases, 74 (59.7%), lived with extended family members compared to 62 (48.4%) controls, though this difference was not statistically significant (p =0.074).Regarding formal education, 20 (16.1%) cases had no education, which was comparable to the control group where 19 (14.8%) had no education. Concerning monthly family income, 38 (30.6%) cases declined to disclose this information.
The overall mean FDRS among cases was 2.51±0.90, and among controls, it was 2.22±1.01. The mean WDDS was 4.77±1.51 for cases and 4.90±1.62 for controls, indicating poor dietary diversity in both groups. Differences between cases and controls were analysed using independent samples t-tests, as presented in Table II.
Table II: Comparison of FDRS, WDDS and anthropometric measures between cases and controls
|
Parameters |
Cases |
Control |
p-value |
|
Mean ± SD |
Mean ± SD |
||
|
FDRS |
2.51 ± 0.90 |
2.22 ± 1.01 |
0.048 |
|
WDDS |
4.77 ± 1.51 |
4.90 ± 1.62 |
0.531 |
|
Weight (Kg) |
70.05 ±14.83 |
71.09 ± 12.69 |
0.554 |
|
Height (m) |
1.51 ± 0.11 |
1.57 ± 0.11 |
0.069 |
|
BMI (Kg/m2) |
29.62 ± 6.89 |
29.04 ± 6.10 |
0.524 |
|
Waist circumference (cm) |
79.40 ± 28.75 |
80.79 ± 25.71 |
0.740 |
|
Hip Circumference (cm) |
82.86 ± 30.36 |
88.11 ± 26.21 |
0.229 |
|
Waist to hip ratio |
0.97 ± 0.24 |
0.92 ± 0.19 |
0.138 |
p-value calculated using an Independent T-test'BMI:Body mass index; FDRS:Finnish Diabetes Risk Score; WDDS:Women’s Diet Diversity
The analysis revealed that cases had significantly higher FDRS compared to controls (p =0.048). However, waist and hip circumferences were lower in cases compared to controls, while no significant differences were observed for BMI and WDDS between the two groups. Overall, more than half of the participants in both groups fell into the WHO category of high risk for chronic disease with a BMI >29 kg/m².
Stratified analysis showed that mean FDRS was significantly higher among cases with WDDS <5 and BMI >27.5 kg/m² compared to controls (Figure 1a and 1b).
Overall, both the cases and control groups showed limited dietary diversity. On dialysis days, 9% of participants reported skipping lunch. For breakfast, roti or paratha (a type of fried bread) with tea was commonly consumed in both groups. Lunch and dinner typically consisted of vegetable or lentil curry, and tea with milk was the most commonly consumed beverage throughout the day. Due to cost considerations, meat, predominantly chicken or beef, was consumed infrequently. Raw vegetables or salads were rarely included in meals, although vegetable curry was reported by 41% of cases and 44% of controls.
There were significant differences in fruit consumption between cases and controls. Only 37.4% of cases reported consuming at least one piece of fruit per day, whereas 47.3% of controls did so (P =0.001).
The results revealed that 61% of cases resided in joint family setups where they received assistance from family members in managing daily household chores while caring for a dialysis-dependent family member. However, becoming a caregiver led to an increase in physical activity outside the home. According to responses to open-ended questions, previously these tasks were typically performed by a male family member, such as grocery shopping or transporting children to school. However, after the care-recipient became dependent on dialysis, these responsibilities shifted to the caregiver, who now handles tasks like market visits and other duties outside the home. Additionally, due to the scheduled visits to the dialysis centre two to three times a week, caregivers took on responsibilities such as purchasing medications. Consequently, caregivers reported an expanded role outside the home, including activities like grocery shopping and visiting mechanics.
The clinical and biochemical markers for chronic disease were compared between the cases and control participants using independent samples t-tests. There were no statistically significant differences between the two groups. However, further stratified analysis was conducted, showing significant associations with FDRS for all variables except triglycerides. Figures 1 (c) to 1 (f) present these findings. The analyses demonstrated that the cases had significantly higher mean FDRS, suggesting an elevated risk of developing T2DM.
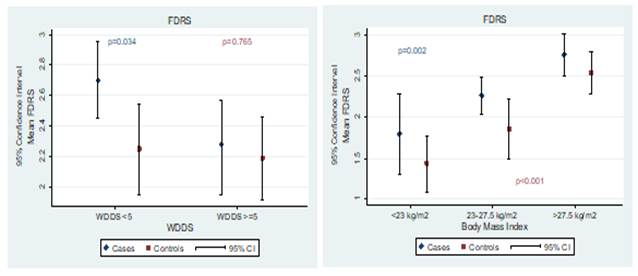
Figure 1(a): Comparison of mean FDRS and WDDS between cases and controls.
Figure 1 (b): Comparison of mean FDRS and BMI between cases and controls.
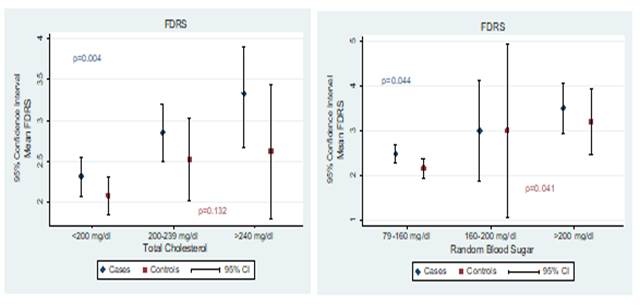
Figure 1 (c): Comparison of mean FDRS and total cholesterol between cases and controls.
Figure 1 (d): Comparison of mean FDRS and random blood glucose between cases and controls.
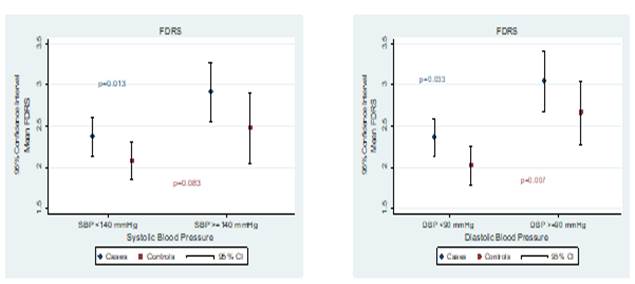
Figure 1 (e): Comparison of mean FDRS and systolic blood pressure between cases and controls.
Figure 1 (f): Comparison of mean FDRS and diastolic blood pressure between cases and controls.
……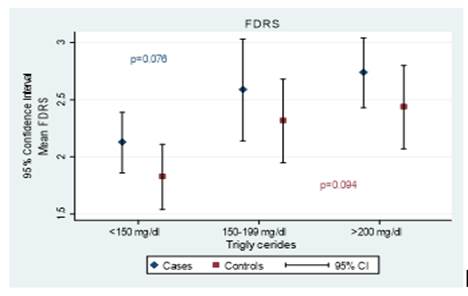
Figure 1 (g): Comparison of mean FDRS and triglycerides between cases and controls.
DISCUSSION
Caregivers are often seen as informal healthcare providers, yet their own health and daily lifestyle can suffer, potentially increasing their vulnerability to chronic diseases.3,13 This study represents the first attempt to compare diet, physical activity, biochemical markers of chronic disease, and the risk of developing T2DM using the FDRS among female caregivers of dialysis-dependent patients in Pakistan. Although no significant differences were detected in the biochemical markers of chronic disease, the comprehensive evaluation with FDRS, encompassing lifestyle factors and family history, revealed that caregivers (cases) face an increased risk of developing T2DM compared to controls. This highlights the importance of healthcare professionals, policymakers, and society addressing the health and well-being of caregivers.
In Pakistan, obesity poses a significant public health challenge, with over 40% of women of reproductive age classified as overweight or obese.19 The study results indicated no significant differences in anthropometric measurements between the cases and controls; however, more than 50% of women in both groups were categorized as obese. Previous research has documented weight changes among caregivers.20,21 For instance, Vitaliano PP, et al., reported weight gain in female caregivers compared to controls in a case-control study.21 Interestingly, in the current study, both groups were found to be obese. The prevalence of obesity among caregivers may stem from factors such as limited time for preparing healthy meals or increased food intake due to compromised mental health. Therefore, prospective cohort studies are warranted to elucidate whether care giving roles contribute to weight gain over time.
Biochemical tests can complement anthropometric measurements in assessing the risk of chronic disease. Results from total cholesterol and random blood glucose levels indicated that participants in both groups were categorized as "low risk" for chronic diseases. However, triglyceride levels were observed to be in the "high-risk" category for both groups. This finding highlights the need for further investigation to determine whether elevated triglyceride levels are associated with dietary intake or genetic predisposition.22
It is widely reported that the diet of caregivers is adversely affected by their role. 6, 20,21 In our study, 46% of the cases reported a decreased food intake since becoming caregivers. The major reasons reported for the reduced food intake were decrease in appetite, lack of time for food preparation on dialysis days and limited choice due to the necessity of consuming only those food items which the dialysis-dependent family member consumed. Similar findings have been reported by the caregivers looking after family members living with other chronic diseases as well.6,20,21,22 For example in a study conducted in the UK, caregivers reported to prefer consumption of food items suggested to their dependent family member living with cancer, to improve dietary compliance of patient.23 Similarly, using qualitative approach a study was conducted to assess the experience of caregivers of immigrants who were dependent on haemodialysis highlighted that caregivers tend to avoid foods which are not suitable for HD-dependent patients.24
The cases and controls represent poor diet diversity with the mean WDDS falling below 5. It is worth to note that the WDDS score was positively associated with FDRS. This finding is consistent with the recently published study conducted in Pakistan. The data was collected from women of reproductive age (non-pregnant and non-lactating). Data was collected five times in a year (to consider seasonal variation) using 24-hour dietary recall. Results indicated that the mean food group diversity score of the participants was 4±1, and only 26% and 41% of women achieving a minimum dietary diversity for women score of 5.25
Similarly, recently published Pakistan Dietary guidelines for better Nutrition, two to three servings from fruits and vegetable (from each food group) are recommended per day. However, this is rarely achieved, which can be due to a low literacy, limited financial resources and lack of awareness regarding its benefits or due to the high cost of fruit. 26-28 Moreover, Safdar NF, et al., reported results from COBRA trial that high intake of fruits and vegetable are found among Pakistani population who are educated, physically active and non-tobacco users. 28 Thus, there is need for health promotion programs to promote health literacy among caregivers keeping in view their daily responsibilities.
One major strength of our study is that, to our best knowledge, it is the first to investigate the relationship between diet, physical activity, and chronic disease risk among caregivers of haemodialysis-dependent patients in Pakistan. The chosen control group consisted of female caregivers attending to family members with acute illnesses like fever at the same hospital. This comparison is advantageous as both groups are likely from similar socio-economic backgrounds.
The results of our study can gain the attention of the healthcare professionals and the policy makers to design and implement the health promotion programs targeting the female caregivers for skills and possible challenges relating to the long term care of haemodialysis patients. This may include such skills for cost-effective grocery, preparing a modified diet, monitoring vital signs (such as body temperature and blood pressure), hygiene skills (such as giving bath to the care-recipient), managing fistula and catheter. In addition to caregiver, such programs can benefit to other stakeholders, such as care-recipients and health professionals.
Our study has several limitations that should be considered. Convenience sampling was employed, potentially limiting the generalizability of the findings, as stated by Pruchno RA, et al.29 Additionally, data collection was conducted in Rawalpindi, a metropolitan city in Pakistan. This could be viewed as a limitation due to environmental factors, such as higher levels of education and employment opportunities, especially for females, typically found in such cities. Therefore, the sample may not fully represent the broader population of Pakistan. However, it is noteworthy that 25% of the participants resided in cities other than Rawalpindi, which helps mitigate potential selection bias to some extent.
The data collection took place within a hospital setting, where typically only one caregiver accompanies the patient. Consequently, data was provided by the caregivers visiting the dialysis centre, but it might have been more beneficial to gather data from other family members of the care recipients. Moreover, due to the participants' low literacy rates and limited understanding of research processes such as consent forms and Likert scales, it was challenging to obtain high-quality quantitative data.
Another limitation pertained to incomplete data, particularly in terms of blood samples and waist and hip circumference measurements, due to cultural sensitivities. This aspect should be considered in the planning of future studies conducted within this cultural context. It also raises concerns about the appropriateness of using data collection tools designed and validated in Western cultures within the Pakistan context.
CONCLUSION
This study indicates that both cases and controls exhibit similar risk factors for chronic diseases, including poor diet diversity with low fruit intake, high BMI and central adiposity, and elevated blood triglyceride levels. Although the overall risk score for developing T2DM was generally low, it was slightly higher in the cases compared to the controls. Given the average age of the participants at 40 years, tracking the long-term health outcomes influenced by the care giving role would be beneficial.
Moreover, the study underscores the necessity for culturally appropriate health promotion programs, as well as leadership and advocacy from healthcare professionals. These initiatives are crucial in promoting healthy lifestyles among this vulnerable caregiving group and the broader population.
REFERENCES
1. Hughes N, Locock L, Ziebland S. Personal identity and the role of ‘carer’among relatives and friends of people with multiple sclerosis. Soc Sci Med 2013;96:78-85. https://doi.org/10.1016/j.socscimed.2013.07
2. https://doi.org/10.1016/j.socscimed.2013.07.023
3. Highet NJ, McNair BG, Davenport TA, Hickie IB. “How much more can we lose?”: carer and family perspectives on living with a person with depression. Med J Aust 2004;181:S6-S9.
4. Schulz R, Beach SR. Caregiving as a risk factor for mortality: the caregiver health effects study. JAMA 1999;282(23):2215-9.
5. Butow PN, Price MA, Bell ML, Web PM, deFazio A, Australian Ovarian Cancer Study Group, et al. Caring for women with ovarian cancer in the last year of life: a longitudinal study of caregiver quality of life, distress and unmet needs. Gynecol Oncol 2014;132(3):690-97. https://doi.org/10.1016/j.ygyno.2014.01.002
6. Mohanty I, Niyonsenga T. A longitudinal analysis of mental and general health status of informal carers in Australia. BMC Public Health 2019;19(1):1436. https://doi.org/10.1186/s12889-019-7816-8
7. Warren R, Lambert S, Razee H. The dietary behaviours of cancer caregivers: preliminary findings on how becoming a cancer caregiver might influence food choices and dietary behaviours in the carer compared with pre-caring. J Glob Oncol 2018;4(Supply 2):33000.https://doi.org/10.1200/jgo.18.33000
8. Mochari-Greenberger H, Mosca L. Caregiver burden and nonachievement of healthy lifestyle behaviors among family caregivers of cardiovascular disease patients. Am J Health Promot 2012;27(2):84-9. https://doi.org/10.4278/ajhp.110606-quan-241
9. Minhas A, Vajaratkar V, Divan G, Hamdani SU, Leadbitter K, Taylor C, et al. Parents' perspectives on care of children with autistic spectrum disorder in South Asia - Views from Pakistan and India. Int Rev Psychiatry 2015;27(3):247-56. https://doi.org/10.3109/09540261.2015.1049128
10. Mirza I, Tareen A, Davidson LL, Rahman A. Community management of intellectual disabilities in Pakistan: a mixed methods study. J Intellect Disabil Res 2009;53(6):559-70. https://doi.org/10.1111/j.1365-2788.2009.01176.x
11. Bikbov B, Purcell CA, Levey AS, Smith M, Abdoli A, Abede M, et al. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020;395(10225):709-33. https://doi.org/10.1016/s0140-6736(20)30045-3
12. Shafi ST, Saleem M, Anjum R, Abdullah W, Shafi T. Refusal of hemodialysis by hospitalized chronic kidney disease patients in Pakistan. Saudi J Kidney Dis Transpl 2018;29(2):401-8. https://doi.org/10.4103/1319-2442.229270
13. Cantekin I, Kavurmacı M, Tan M. An analysis of caregiver burden of patients with hemodialysis and peritoneal dialysis. Hemodial Int 2016;20(1):94-7.https://doi.org/10.1111/hdi.12311
14. Arora S, Rechel B, Bergland A, Straiton M, Debesay J. Female Pakistani carers' views on future formal and informal care for their older relatives in Norway. BMC Health Serv Res 2020;20(1):603. https://doi.org/10.1186/s12913-020-05468-z
15. Al-Mawali A, Jayapal SK, Morsi M, Al-Shekaili W, Pinto AD, Al-Kharusi H, et al. Prevalence of risk factors of non-communicable diseases in the Sultanate of Oman: STEPS survey 2017. PLoS One 2021;16(10):e0259239. https://doi.org/10.1371/journal.pone.0259239
16. Tan K. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004;363(9403):157-63.https://doi.org/10.1016/s0140-6736(03)15268-3
17. FAO F. Minimum dietary diversity for women: a guide for measurement. Rome: FAO. 2016;82. [Accessed on: June 06, 2024]. Available from URL: https://www.fao.org/nutrition/assessment/tools/minimum-dietary-diversity-women/en/
18. Bergmann A, Li J, Wang L, Schulze J, Bornstein S, Schwarz P. A simplified Finnish diabetes risk score to predict type 2 diabetes risk and disease evolution in a German population. Horm Metab Res 2007;39(09):677-82. https://doi.org/10.1055/s-2007-985353
19. Omech B, Mwita JC, Tshikuka J-G, Tsima B, Nkomazna O, Amone-P’Olak K. Validity of the Finnish Diabetes Risk Score for detecting undiagnosed type 2 diabetes among general medical outpatients in Botswana. Journal of diabetes research. 2016;2016.
20. Satti MN, Durr-e-Nayab, Khalid M. Prevalence and determinants of overweight and obesity among adults in Pakistan. [Accessed on: January 21, 2019]. Available from URL: https://file.pide.org.pk/pdfpideresearch/phwps-002-prevalence-and-determinants-of-overweight-and-obesity-among-adults-in-pakistan.pdf
21. Beesley VL, Price MA, Webb PM, Group AOCS, Investigators AOCSQoLS. Loss of lifestyle: health behaviour and weight changes after becoming a caregiver of a family member diagnosed with ovarian cancer. Support Care Cancer 2011;19:1949-56. https://doi.org/10.1007/s00520-010-1035-2
22. Vitaliano PP, Russo J, Scanlan JM, Greeno CG. Weight changes in caregivers of Alzheimer's care recipients: psychobehavioral predictors. Psychol Aging 1996;11(1):155. https://doi.org/10.1037//0882-7974.11.1.155
23. Galicia-Garcia U, Benito-Vicente A, Jebari S, Larrea-Sebal A, Siddiqi H, Uribe KB, et al. Pathophysiology of type 2 diabetes mellitus. Int J Mol Sci 2020;21(17):6275. https://doi.org/10.3390/ijms21176275
24. Patterson J, Rapley T, Carding P, Wilson JA, McColl E. Head and neck cancer and dysphagia; caring for carers. Psychooncology 2013;22(8):1815-20. https://doi.org/10.1002/pon.3226
25. Cervantes L, Carr AL, Welles CC, Zoucha J, Steiner JF, Johnson T, et al. The experience of primary caregivers of undocumented immigrants with end-stage kidney disease that rely on emergency-only hemodialysis. J Gen Intern Med 2020;35:2389-97. https://doi.org/10.1007/s11606-020-05696-3
26. Brazier AKM, Lowe NM, Zaman M, Shahzad B, Ohly H, McArdle HJ, et al. Micronutrient status and dietary diversity of women of reproductive age in rural Pakistan. Nutrients. 2020 Nov 6;12(11):3407. https://doi.org/10.3390/nu12113407)
27.; Pitt E, Gallegos D, Comans T, Cameron C, Thornton L. Exploring the influence of local food environments on food behaviours: a systematic review of qualitative literature. Public Health Nutr 2017;20(13):2393-2405. https://doi.org/10.1017/s1368980017001069
28. Amjad M, Akbar M. The association between fruit and vegetable intake and socioeconomic factors in the households of pakistan using quantile regression model. Soc Work Public Health 2023;38(3):248-58. https://doi.org/10.1080/19371918.2022.2134249
29. Safdar NF, Bertone-Johnson E, Cordeiro L, Jafar TH, Cohen NL. Dietary patterns of Pakistani adults and their associations with sociodemographic, anthropometric and life-style factors. J Nutr Sci 2013;2:e42. https://doi.org/10.1017/jns.2013.37
30. Pruchno RA, Brill JE, Shands Y, Gordon JR, Genderson MW, Rose M, et al. Convenience samples and caregiving research: how generalizable are the findings? Gerontologist 2008;48(6):820-27. https://doi.org/10.1093/geront/48.6.820
AUTHORS' CONTRIBUTIONS Following authors have made substantial contributions to the manuscript as under: SN: Concept and study design, acquisition, analysis and interpretation of data, drafting the manuscript, approval of the final version to be published NML, VHM & SD: Concept and study design, analysis and interpretation of data, drafting the manuscript, critical review, approval of the final version to be published SZ: Analysis and interpretation of data, drafting the manuscript, approval of the final version to be published Authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST Authors declared no conflict of interest, whether financial or otherwise, that could influence the integrity, objectivity, or validity of their research work. GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |