![]() https://doi.org/10.35845/kmuj.2024.23448 CLINICAL TRIAL
https://doi.org/10.35845/kmuj.2024.23448 CLINICAL TRIAL
Comparative effects of dry needing and cross friction massage on pain, mobility and functional status in plantar fasciitis: a randomized clinical trial
Kashaf Ziaullah ![]() 1 , Saleh Shah 1,
Muhammad Naveed Babur
1 , Saleh Shah 1,
Muhammad Naveed Babur ![]() 1, Javaria Sharif
1, Javaria Sharif ![]() 1, Kashan Ahmed
1, Kashan Ahmed ![]() 1 , Faiza Gulzar
1 , Faiza Gulzar ![]() 1 , Fatima Chaudhry
1 , Fatima Chaudhry ![]() 1
1
|
1: Department of Physical Therapy, Superior University, Lahore, Pakistan
Email Contact #: +92-331-6339007
Date Submitted: August 17, 2023 Date Revised: November 05, 2024 Date Accepted: November 11, 2024 |
|
THIS ARTICLE MAY BE CITED AS: Ziaullah K, Shah S, Babur MN, Sharif J, Ahmed K, Gulzar F, et,al. Comparative effects of dry needing and cross friction massage on pain, mobility and functional status in plantar fasciitis: a randomized clinical trial. Khyber Med Univ J 2024;16(4): 302-7. https://doi.org/10.35845/kmuj.2024.23448 |
ABSTRACT
Objectives: To compare the effectiveness of dry needling (DN) and cross-friction massage (CFM) in reducing pain and improving mobility and functional status in patients with plantar fasciitis.
Methods: This randomized clinical trial was conducted from January 15 to June 20, 2023, on 48 patients fulfilling the inclusion criteria. Data were collected from Health City Hospital, Tabba Clinic, and Liaqat Physiotherapy Clinic, Lahore-Pakistan. Patients were randomized through lottery method into two groups (n=24 each), receiving either DN or CFM for 8 weeks with 2 sessions per week. Pain, foot health, and functional status were assessed pre- and post-treatment using the Pain Scale for Plantar Fasciitis (PSPF), Foot Health Status Questionnaire (FHSQ), and Foot Functional Index (FFI). Data were analyzed using SPSS-22.
Results: Data were nonparametric, comprising 15 males (31.3%) and 33 females (68.7%), with a mean age of 33.9±2.88 years. Both groups showed significant improvements in pain, mobility, and functional status post-intervention (p =0.001 for PSPF, FHSQ, and FFI). However, DN demonstrated greater effectiveness compared to CFM, with higher post-treatment mean ranks for PSPF (85.4 vs. 74.6), FHSQ (88.2 vs. 72.3), and FFI (92.5 vs. 68.5; p < 0.001). Across-group Wilcoxon T test results indicated significant z-score changes (-4.4 to -4.2), and Mann-Whitney U test comparisons showed significant shifts (97.5 to 145.5). The DN group achieved a mean change of 15.44.
Conclusion: DN is more effective than CFM for pain reduction, mobility improvement, and functional enhancement in plantar fasciitis. Further studies with larger, more diverse populations and longer follow-up are recommended.
Clinical trial registration number: NCT05915091
Keywords: Cross friction massage (Non-MeSH); Dry Needling (MeSH); Functional Status (MeSH); Heel pain (Non-MeSH); Mobility (MeSH); Mobility Limitation (MeSH); Pain (MeSH); Fasciitis, Plantar (MeSH).
INTRODUCTION
Plantar fasciitis is a degenerative condition affecting the fascia on the plantar aspect of the foot, characterized by sub-acute or chronic heel pain at the attachment of the medial band to the medial calcaneal tubercle. 1 Symptoms commonly include severe pain in the medial calcaneus, particularly during the first steps in the morning or after prolonged rest, and are often aggravated by weight-bearing activities. 2 However, activity following rest may also exacerbate the condition.3
Plantar fasciitis accounts for approximately 80% of heel pain cases and affects around 10% of the general population, with 20-30% of patients reporting bilateral symptoms. 4 Globally, an estimated 1 million new cases are diagnosed annually. The prevalence is highest in individuals aged 45-64 years and lowest in those aged 18-25 years, with females being 2.5 times more likely to develop the condition than males. 5
This condition is associated with intense pain, reduced mobility, impaired functional status, diminished quality of life, limited range of motion, and other functional deficits. Pain, mobility issues, and functional status impairment are the most significantly affected aspects of a patient’s health, severely impacting their quality of life and ability to function.
Despite its significant impact, the optimal treatment for plantar fasciitis remains unclear.6 Treatment protocols have evolved over time, ranging from exercise and icing to the use of NSAIDs for pain relief. Cross-friction massage and stretching of the plantar fascia, Achilles tendon, soleus, and gastrocnemius are integral to conservative treatment.7 Combined conservative and invasive approaches are often more effective, with surgical intervention reserved for cases unresponsive to non-surgical methods.8
A key research gap involves insufficient time frames in prior studies to evaluate the short- and long-term effects of dry needling. Earlier protocols used only 3 weeks with one session per week.9,10 This study extends the duration to 8 weeks with two sessions per week to better assess pain reduction and mobility improvement.
The rationale for this study was to identify the more effective treatment between dry needling (DN) and cross-friction massage (CFM) for plantar fasciitis. The study was planned to provide robust evidence for patients and physical therapists, enabling the selection of a treatment that addresses the debilitating symptoms of plantar fasciitis while offering sustained long-term relief.
METHODS
This randomized clinical trial was conducted from January 15 to June 20, 2023, on 48 patients fulfilling the inclusion criteria. Data were collected from Health City Hospital, Tabba Clinic, and Liaqat Physiotherapy Clinic, Lahore-Pakistan.
The sample size was calculated using the OpenEpi tool, resulting in a total of n=48n = 48n=48, with 24 participants in each group.
The parameters for the sample size calculation were as follows:
- Level of significance: Z1-α/2 = 95%
- Power of the study: Z1-β= 80%
- Expected mean change in Group A: µ1= 61
- Expected mean change in Group B: µ2=50.9
- Expected standard deviation in Group A: δ1=10.3
- Expected standard deviation in Group B: δ2= 14
Based on these parameters, the expected sample size in each group was determined to be 24 participants.
A non-probability convenience sampling technique was employed for this study.
Eligibility criteria:
The inclusion criteria consisted of:
· Patients older than 18 years of age.
· Ability to understand the instructions and questions provided during the assessment.
· Patients experiencing pain during the first steps in the morning for at least one month.
· Ability to walk 50 meters without support.
· Willingness to stop the use of NSAIDs, paracetamol, or other analgesics at least two weeks prior to the initial evaluation.6,7,11
The exclusion criteria included:
· Fear of needles
· Refusal to undergo physical therapy sessions as advised
· Current use of anticoagulants
· Presence of chronic diseases, such as rheumatoid arthritis, neurological abnormalities, septic arthritis, ankylosing spondylitis, or sciatica
· History of plantar fascia surgery
· Pregnancy
Ethical considerations: Informed consent was obtained from all participants. Patient identity and personal information were kept strictly confidential. Anonymity of the participants was maintained throughout and after the study. Participants were informed of their right to withdraw from the study at any time. All data were securely stored to ensure privacy and compliance with ethical standards.
Patient selection and randomization: Patients meeting the inclusion criteria were selected from hospital and clinical settings in Lahore-Pakistan. Details of patient enrollment, intervention allocation, and follow-up are presented in the CONSORT flowchart (Figure 1).
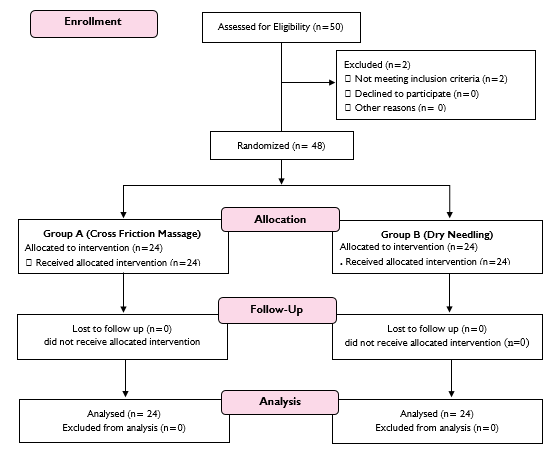
Figure 1: CONSORT Flow chart showing enrollment, intervention allocation and follow-up
Randomization was achieved through the lottery method. Patients with plantar fasciitis were randomly allocated to groups A and B using opaque sealed envelopes containing treatment options. Each patient randomly selected an envelope to determine their assigned intervention. Before treatment administration, a thorough evaluation was conducted, including demographic data, medical and personal history, pain assessment, and functional scale evaluation. Foot health was assessed using the Foot Health Status Questionnaire (FHSQ), pain intensity was evaluated using the Pain Scale for Plantar Fasciitis (PSPF), and functional status was measured using the Foot Functional Index (FFI).
Assessment tools:
Foot health status questionnaire (FHSQ):
- The FHSQ comprises 13 questions across four domains: pain (4 questions), function (4 questions), footwear (3 questions), and general foot health (2 questions).12
- Scores were transformed to a 0–100 scale for each domain, with higher scores reflecting better foot health and quality of life. The FHSQ has been validated and widely used in similar trials evaluating plantar heel pain interventions.
Foot functional index (FFI):
- The FFI consists of 23 questions divided into three subcategories: pain (9 questions), disability (9 questions), and activity limitation (5 questions).13
- Each question is scored from 0 (no pain/limitation) to 10 (worst pain/limitation). This tool is reliable and validated for assessing functional status.
Plantar fasciitis pain scale (PFPS):
- The PFPS includes 20 questions addressing pain and mobility problems specifically related to plantar fasciitis. Scores range from 0 (least occurrence) to 3 (repeated occurrence).14,15
Interventions:
Dry needling:
- Thin monofilament needles (0.16 × 25 mm) were used without injectables. Needle length varied from 30–50 mm, based on the location of myofascial trigger points (MTrPs), with diameters between 0.25 mm and 0.30 mm.
- Rapid needle entry and exit were performed to elicit a local twitch response (LTR), lasting approximately 5 seconds at a rhythmic rate of 1 Hz/second, with five entries per session. The number of LTRs was recorded. After use, needles were discarded, and the insertion site was compressed for 10 seconds to minimize sensitivity.
Cross friction massage:
- The procedure began with circular motions over the ball of the foot and the base of the toes.
- The therapist used both hands to massage the arch, applying pressure with the heel of the hand along the sole.
- Each toe was gently pulled away from the foot, starting with the big toe. The massage concluded with circular rubbing of the heel.
Data analysis: Data were analyzed using SPSS version 26. Normality of pre- and post-intervention data was assessed using the Shapiro-Wilk and Kolmogorov-Smirnov tests.
- Between-group comparison: Conducted using the Wilcoxon Rank Sum Test.
- Within-group comparison: Conducted using the Mann-Whitney U test.
RESULTS
The data were analyzed using SPSS version 22. Tests of normality, including the Kolmogorov-Smirnov and Shapiro-Wilk tests, indicated a non-significant p-value (>0.05), confirming that the data were not normally distributed. Therefore, non-parametric tests were applied.
The mean age of participants was 33.9±2.88 years. The study population included 8 males (31.3%) and 33 females (68.7%). Side involvement showed 23 patients (47.9%) with left-side involvement and 25 patients (52.1%) with right-side involvement. The mean duration of symptoms was 2.21±0.74 months. The mean weight of the participants was 72.4±8.9 kg. Over half of the study participants, 56.26% (n=27), were classified as obese with a BMI of ≥30 kg/m² (Table I).
Table II shows significant post-treatment improvements in pain, foot health, and functionality in both groups. Median scores for the PSPF, FHSQ, and FFI decreased significantly in both the dry needling group (Group A) and the cross-friction massage group (Group B) (p=.001 for all measures). Both interventions effectively reduced symptoms and improved foot health and functionality.
Significant differences were observed between dry needling and cross-friction massage in terms of pain, foot health, and functionality both before and after treatment, as shown in Table III. For the PSPF, post-treatment median and mean ranks improved significantly in both groups (p = 0.001), with DN achieving a higher mean rank of 85.4 compared to CFM's 74.6. Similarly, the FHSQ indicated statistically significant post-treatment improvements favoring DN, which had a lower median (30) and higher mean rank (88.2) than CFM (median: 40; mean rank: 72.3) (p < 0.001). The FFI scores also showed significant enhancements for both interventions, with DN exhibiting greater effectiveness, reflected by a mean rank of 92.5 compared to 68.5 for CFM (p < 0.001). These results emphasize the effectiveness of both techniques, with DN demonstrating marginally superior improvements across all measured outcomes.
Table I: Demographics of the study sample
|
Variables |
Frequency (n=48) |
Percentage |
|
|
Gender |
Male |
15 |
31.3 |
|
Female |
33 |
68.7 |
|
|
Side |
Left |
23 |
47.9 |
|
Right |
25 |
52.1 |
|
|
Body mass index (kg/m2) |
Normal (18.5-24.9) |
3 |
6.25 |
|
Over weight (25-29.9) |
18 |
37.5 |
|
|
Obese (30 onwards) |
27 |
56.26 |
|
Table II; Comparison of pre- and post-treatment outcomes for dry needling and cross-friction massage in plantar fasciitis
|
Variables |
Group A (dry needling) |
Group B (cross friction massage) |
||||||||||
|
Median (IQR) |
Mean difference |
Z score |
Mean rank |
p-value |
Median (IQR) |
Mean difference |
Z score |
Mean rank |
p-value |
|
||
|
PSPF |
Pre |
51 (4) |
19 |
-4.22 |
26.19 |
.001 |
49 (3) |
14 |
-4.4 |
22.81 |
.001 |
|
|
Post |
32 (3) |
22.35 |
35(3) |
21.65 |
|
|||||||
|
FHSQ |
Pre |
85(13) |
35 |
-4.22 |
16.56 |
.001 |
88 (2) |
30 |
-4.4 |
16.44 |
.001 |
|
|
Post |
50 (15) |
13.56 |
58 (3) |
15.71 |
|
|||||||
|
FFI |
Pre |
65 (4) |
6 |
-4.2 |
16.63 |
.001 |
69 (3) |
4 |
-4.4 |
32.38 |
.001 |
|
|
Post |
59 (5)
|
12.71 |
65 (3)
|
32.29 |
|
|||||||
PSPF=Pain Scale for Plantar Fasciitis; FHSQ=Foot Health Status Questionnaire; FFI=Foot Functional Index
Table II: comparison of dry needling and cross-friction massage outcomes using the mann-whitney u test
|
Variables |
Pre treatment |
Post treatment |
|
||||||
|
Median (IQR) |
Mean Rank |
Mann-Whitney U value |
p value |
Median (IQR) |
Mean Rank |
Mann-Whitney U value |
p-value |
||
|
PSPF* |
DN |
51 (4) |
26.19 |
247.5 |
0.001 |
51 (4) |
22.35 |
267.5 |
0.001 |
|
CFM |
49 (3) |
22.81 |
49 (3) |
23.65 |
|||||
|
FHSQ* |
DN |
85 (13) |
16.56 |
97.5 |
<0.001 |
50 (19) |
32.44 |
145.5 |
.001 |
|
CFM |
88 (2) |
16.44 |
88 (2) |
18.56 |
|||||
|
FFI* |
DN |
65(4) |
16.63 |
99.0 |
<0.001 |
60 (5) |
612.71 |
101.0 |
<0.001 |
|
CFM |
69 (3) |
32.38 |
65(3) |
32.29 |
|||||
PSPF=Pain Scale for Plantar Fasciitis; FHSQ=Foot Health Status Questionnaire; FFI=Foot Functional Index; DN=dry needling; CFM= cross friction massage
DISCUSSION
This study evaluates and compares two widely recognized treatment approaches for plantar fasciitis: CFM and DN. A total of 48 patients with plantar fasciitis were randomized into two groups, receiving DN and CFM interventions, respectively. The results demonstrated that the DN group showed significantly greater improvements in pain, mobility, and functional status compared to the CFM group. For instance, the DN group achieved higher mean ranks in PSPF (85.4 vs. 74.6, p = 0.001), FHSQ (mean rank: 88.2 vs. 72.3; p < 0.001), and FFI (mean rank: 92.5 vs. 68.5; p < 0.001). These findings highlight the superior efficacy of DN in alleviating pain and enhancing foot health and functionality, although both interventions produced statistically significant improvements post-treatment.
In 2021 Saein et al15 conducted research to study the effects of dry needling on ROM, pain, and changes observed ultrasonographically in plantar fascia. PFPS (P = .03) is decreased. However, there was no difference in plantar flexion and dorsiflexion range of motion. In contrast to the recent study the improvement in pain scale was less after due to the smaller number of patients (n=20) to study the effect.8 Rahber et al compared electric shockwave therapy with DN (dry needling) and concluded that both techniques were effective in improving pain in plantar fasciitis he discussed the comparative effects of dry needling effect in addition to extracorporeal shock wave. This research determined that together ESWT plus dry needling remained operative in plantar fasciitis however dry needling is more effective in producing effects in the long term i.e. 8 weeks in this case.16
Cotchett et al concluded that dry needling is a reliable technique for improving overall foot health and mobility in plantar fasciitis.5 In 2022 Wheeler et al18 investigated the improvement in outcomes after dry needling in comparison to autologous blood injection in plantar fasciitis there was no obvious difference between the groups, and dry needling gave similar effects in improving mobility and foot health. The study concluded that the use of ABI (autologous blood injection) for chronic plantar fasciitis had no significant difference from using dry needling alone, as a whole both of the methods are equally beneficial for the treatment hence the results were consistent with the recent study.
Farooq N et al19 studied the effectiveness of trans friction massage and calf stretching on PF patients. They concluded that both techniques were equally effective in PF with p >0.05 on FFI.16 Jan et al did a study on the comparison of ESWT and stretching with massage and a significant difference in FFI was observed. In contrast to the recent study Bagcier et al suggested that DN only provides better results on FFI when used in combination with ESWT. P=0.2. This study did not include the long-term effects of DN on PF and only comprised one 1 month of treatment, hence the results.20
In 2022, Salehi et al.21 conducted a single-blinded randomized controlled trial to examine the effects of dry needling combined with stretching exercises versus stretching exercises alone on pain intensity and sonographic characteristics in patients with plantar fasciitis. This study concluded that the experimental group showed comparatively better outcomes. In contrast, the current study reported a more pronounced mean change of 15.44 between the two groups. This statistical difference may be attributed to the differing treatment durations, as Salehi et al.'s study implemented a six-week treatment protocol, whereas the current study extended the intervention period to eight weeks. The longer treatment duration in the recent study likely allowed for a more comprehensive assessment of long-term effects, leading to greater improvements in the outcomes.
Limitations of the study
The main limitations of this study include the lack of long-term follow-up, potential bias from subjective pain assessments and unblinded participants, a small sample size, and a single-center design. The use of a nonprobability sampling technique, due to the limited patient pool, further restricts the generalizability of the findings. Additionally, the study did not examine the prevalence of plantar fasciitis across genders. The absence of a control group and the exclusion of other treatment options also limit the scope and applicability of the results. Future research should aim to address these limitations to enhance the robustness and generalizability of the findings.
CONCLUSION
This study demonstrated significant findings favoring Dry Needling over Cross-Friction Massage for the treatment of plantar fasciitis, with DN showing greater reductions in pain and superior improvements in mobility and functional status. While both groups experienced improvements, the DN group exhibited statistically significant superiority, suggesting that DN may be a more effective intervention for managing plantar fasciitis. To enhance the generalizability of these findings, further research using larger, more diverse samples and probability sampling techniques is recommended. Such studies would provide more precise and unbiased results, contributing to a better understanding of effective treatment approaches for plantar fasciitis.
REFERENCES
1. Morrissey D, Cotchett M, Said J'Bari A, Prior T, Griffiths IB, Rathleff MS, et al. Management of plantar heel pain: a best practice guide informed by a systematic review, expert clinical reasoning and patient values. Br J Sports Med 2021;55(19):1106-18. https://doi.org/10.1136/bjsports-2019-101970
2. Naterstad IF, Joensen J, Bjordal JM, Couppé C, Lopes-Martins RAB, Stausholm MB. Efficacy of low-level laser therapy in patients with lower extremity tendinopathy or plantar fasciitis: systematic review and meta-analysis of randomised controlled trials. BMJ Open 2022:28;12(9):e059479. https://doi.org/10.1136/bmjopen-2021-059479
3. Umar H, Idrees W, Umar W, Khalil A, Rizvi ZA. Impact of routine footwear on foot health: A study on plantar fasciitis. J Family Med Prim Care 2022;11(7):3851-5. https://doi.org/10.4103/jfmpc.jfmpc_637_21
4. Holla SS, Srikantaiah S, Debur R. Single Session of Low-dye Calcaneal Taping as a Viable Alternative to LASER Therapy for the Treatment of Plantar Fasciitis: A Randomized Controlled Trial. J Foot Ankle Surg 2022;9(1):31. https://doi.org/10.5005/jp-journals-10040-1182
5. Cotchett M, Lennecke A, Medica VG, Whittaker GA, Bonanno DR.
The association between pain catastrophising and kinesiophobia with pain and
function in people with plantar heel pain. Foot (Edinb) 2017;32:8-14.https://doi.org/10.1016/j.foot.2017.03.003
6. Martin RL, Davenport TE, Reischl SF, McPoil TG, Matheson JW, Wukich DK, et
al. Heel pain-plantar fasciitis: revision 2014. J Orthop Sports Phys Ther 2014;44(11):A1-33.https://doi.org/10.2519/jospt.2014.0303
7.Sahin N, Oztürk A, Atıcı T. Foot mobility and plantar fascia elasticity in
patients with plantar fasciitis. Acta Orthop Traumatol Turc 2010;44(5):385-91.https://doi.org/10.3944/AOTT.2010.2348
8. Khired Z, Najmi MH, Akkur AA, Mashhour MA, Bakri KA. The Prevalence and Risk
Factors of Plantar Fasciitis amongst the Population of Jazan. Cureus 2022:21;14(9):e29434.
https://doi.org/10.7759/cureus.29434
9. Stoychev V, Finestone AS, Kalichman L. Dry Needling as a Treatment Modality
for Tendinopathy: a Narrative Review. Curr Rev Musculoskelet Med 2020;13(1):133-40.
https://doi.org/10.1007/s12178-020-09608-0
10. Al-Boloushi Z, Gómez-Trullén EM, Bellosta-López P, López-Royo MP, Fernández
D, Herrero P. Comparing two dry needling interventions for plantar heel pain: a
protocol for a randomized controlled trial. J Orthop Surg Res 2019:25;14(1):31.https://doi.org/10.1186/s13018-019-1066-4
11. Griswold D, Learman K, Ickert E, Clewley D, Donaldson MB, Wilhelm M, et al.
Comparing dry needling or local acupuncture to various wet needling injection
types for musculoskeletal pain and disability. A systematic review of
randomized clinical trials. Disabil Rehabil 2024;46(3):414-28. https://doi.org/10.1080/09638288.2023.2165731
12. Eftekharsadat B, Babaei-Ghazani A, Zeinolabedinzadeh V. Dry needling in patients with chronic heel pain due to plantar fasciitis: A single-blinded randomized clinical trial. Med J Islam Repub Iran 2016 :23;30:401.
13. Dunning J, Butts R, Henry N, Mourad F, Brannon A, Rodriguez H, et al. Electrical dry needling as an adjunct to exercise, manual therapy and ultrasound for plantar fasciitis: A multi-center randomized clinical trial. PLoS One 2018;31;13(10):e0205405. https://doi.org/10.1371/journal.pone.0205405
14. Yelverton C, Rama S, Zipfel B. Manual therapy interventions in the treatment of plantar fasciitis: A comparison of three approaches. Health SA 2019; 25;24:1244. https://doi.org/10.4102/hsag.v24i0.1244
15. Saein AM, Safavi-Farokhi Z, Aminianfar A, Mortezanejad M. The Effect of Dry Needling on Pain, Range of Motion of Ankle Joint, and Ultrasonographic Changes of Plantar Fascia in Patients With Plantar Fasciitis. J Sport Rehabil 2022:1;31(3):299-304. https://doi.org/10.1123/jsr.2021-0156
16. Rahbar M, Eslamian F, Toopchizadeh V, Jahanjoo F, Kargar A, Dolatkhah N. A comparison of the efficacy of dry-needling and extracorporeal shockwave therapy for plantar fasciitis: a randomized clinical trial. Iran Red Crescent Med J 2018;20(9):e68908. https://doi.org/10.5812/ircmj.68908
17. Hortz BV, Falsone S. A Multisegmental Approach to Dry Needling Plantar Fasciitis: A Case Study. J Sport Rehabil 2022:1;31(4):490-4. https://doi.org/10.1123/jsr.2021-0385
18. Wheeler PC, Dudson C, Gregory KM, Singh H, Boyd KT. Autologous Blood Injection With Dry-Needling vs Dry-Needling Alone Treatment for Chronic Plantar Fasciitis: A Randomized Controlled Trial. Foot Ankle Int. 2022;43(5):646-57. https://doi.org/10.1177/10711007211061365
19. Farooq N, Aslam S, Bashir N, Awan WA, Shah M, Irshad A. Effectiveness of transverse friction massage of Flexor digitorum brevis and Calf muscle stretching in Plantar fasciitis on foot function index scale: A randomized control trial. Isra Med J 2019;1(4):305-9.
20. Bagcier F, Yilmaz N. The Impact of Extracorporeal Shock Wave Therapy and Dry Needling Combination on Pain and Functionality in the Patients Diagnosed with Plantar Fasciitis. J Foot Ankle Surg 2020;59(4):689-93. https://doi.org/10.1053/j.jfas.2019.09.038
21. Salehi S, Shadmehr A, Olyaei G, Bashardoust S, Mir SM. Effects of dry needling and stretching exercise versus stretching exercise only on pain intensity, function, and sonographic characteristics of plantar fascia in the subjects with plantar fasciitis: a parallel single-blinded randomized controlled trial. Physiother Theory Pract 2023;39(3):490-503. https://doi.org/10.1080/09593985.2021.2023930
AUTHORS' CONTRIBUTIONS Following authors have made substantial contributions to the manuscript as under: KZ, MNB * KA : Conception and study design, acquisition of data, drafting the manuscript, approval of the final version to be published SS, JS, FG & FC: Analysis and interpretation of data, critical review, approval of the final version to be published
Authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST Authors declared no conflict of interest, whether financial or otherwise, that could influence the integrity, objectivity, or validity of their research work.
GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |