![]() https://doi.org/10.35845/kmuj.2024.23407 ORIGINAL
ARTICLE
https://doi.org/10.35845/kmuj.2024.23407 ORIGINAL
ARTICLE
Caffeine consumption and voice health of university teachers: a safe bet!
Muhammad
Bilal Bhatti 1,2, Nazia Mumtaz ![]() 1,
Ghulam Saqulain
1,
Ghulam Saqulain ![]() 3
3
|
1: Department of Speech Language Pathology, Faculty of Rehabilitation and Allied Health Sciences, Riphah International University, Islamabad Campus, Pakistan 2: Department of Speech Therapy, Al-Rehman Hospital, Lahore, Pakistan 3: Department of Otorhinolaryngology, Capital Hospital, Post Graduate Medical Institute, Islamabad, Pakistan
Email
Contact #: +92-333- 5101134
Date Submitted: July 13, 2023 Date Revised: August 17, 2024 Date Accepted: August 21, 2024 |
|
THIS ARTICLE MAY BE CITED AS: Bhatti MB, Mumtaz N, Saqulain G. Caffeine consumption and voice health of university teachers: a safe bet!. Khyber Med Univ J 2024;16(3):231-6. https://doi.org/10.35845/kmuj.2024.23407 |
ABSTRACT
OBJECTIVE: To determine the effects of caffeine on the vocal health of university teachers.
METHODS: This cross-sectional study employed a non-probability convenience sampling technique to recruit 362 university teachers from Riphah International University, University of Education, University of Management and Technology, and University of Punjab, Pakistan between January 1, 2022, and June 31, 2022. The sample included both male and female participants aged 25 to 60 years. A Basic Demographic Sheet and the Voice Handicap Index (VHI) were used for data collection. Data were analyzed using SPSS version-22.
RESULTS: Out of 362 university teachers, 239 (66%) were females and majority (n=92/362, 25.4%) were within the 30-35 years’ age group. The majority of university teachers (n=290; 80.11%) in the study were caffeine users. Among them, 196 (54.1%) had severe voice handicaps, with 72 (19.9%) being non-caffeine users. Importantly, all teachers with mild and moderate handicaps were caffeine users (p=0.000). VHI scale, including functional, physical, and emotional subscale scores, as well as total mean scores, were significantly higher among non-caffeine users (p<0.001). Caffeine use was reported by 91.87% of males, compared to 74.06% of females (p<0.001). Additionally, significantly more males and individuals aged 25-40 years were found to be caffeine users (p<0.05). Both gender and age showed a significant correlation with VHI scores (p<0.001).
CONCLUSION: Caffeine consumption does not significantly impact voice handicaps in the Pakistani context. However, gender and age demonstrate a significant correlation with voice handicaps, indicating that these demographic factors play a more crucial role in influencing vocal health.
KEY WORDS: Caffeine users (Non-MeSH); University teachers (Non-MeSH); Voice Handicap Index (Non-MeSH).
INTRODUCTION
Caffeine is a naturally occurring alkaloid found in various plants, with major sources including coffee, tea, guarana berries, and cacao beans. It exerts its effects on multiple systems within the human body, including the brain, gastrointestinal tract, respiratory system, and urinary tract, primarily by stimulating the central nervous system (CNS).¹ Among the chemicals consumed globally, caffeine is one of the most prevalent and widely ingested, with its primary action focused on the CNS. In addition to caffeine itself, its metabolites-paraxanthine, theobromine, and theophylline (4%)-also contribute to its physiological effects.²
Caffeine consumption is widespread across various populations. For instance, a study of U.S. military personnel reported that 15.9% of individuals consumed more than 400 mg of caffeine daily, while 27.3% consumed more than 300 mg per day, with higher consumption observed in males than females.³ Similar investigations into caffeine intake among university teachers are warranted. The most common sources of caffeine include coffee, energy drinks, tea, sodas, chewing gums, and certain medications.³ Among instructors, caffeine is frequently consumed to enhance neurocognitive function, increase alertness, alleviate headaches, and improve physical performance.¹
Azari S, et al., reported a significant prevalence of voice disorders among university professors, with an overall rate of 41%, peaking at 69% in Iran and dropping to 20% in China, where caffeine use was notably high.⁴ Despite this, Franca MC, et al., demonstrated that a 100 mg dose of caffeine had no discernible impact on vocal acoustic or aerodynamic characteristics.⁵ Nonetheless, the voice is a critical tool for educators, directly influencing the learning environment and teaching efficacy.⁶ University teachers are particularly vulnerable to voice-related issues, often stemming from vocal habits that involve increased vocal effort and improper phonation techniques.⁷ These practices can lead to vocal fold tissue damage and vocal fatigue, which, in turn, may negatively affect teaching performance and pedagogical outcomes.
Voice production is a complex physiological process requiring the coordinated function of respiration, phonation, and resonance. The larynx, as the primary structure responsible for voice production, requires diligent care to maintain vocal health. Consequently, preventive vocal hygiene programs are essential to ensure the long-term functionality of the vocal apparatus. ⁸ Due to its diuretic properties, caffeine is often considered a dehydrating agent, potentially disrupting fluid balance in the body. Dehydration is believed to adversely affect phonation, though empirical evidence supporting this claim is limited. ⁹ The lack of reliable data on this topic highlights the need for further research to guide evidence-based practices and develop preventive strategies for caffeine-related voice disorders. ⁹
Given this research gap, the current study was conducted to assess the effects of caffeine on the voice of university teachers within the Pakistani cultural context, where women, in particular, may avoid public smoking due to cultural norms. This study aims to provide baseline knowledge regarding the impact of caffeine consumption on vocal production in university instructors. The findings may prove valuable for voice therapists in developing strategies to optimize vocal function, particularly for individuals with high vocal demands who are regular caffeine users. ¹⁰
METHODS
The present study employed a cross-sectional design with non-probability convenience sampling. A total of 362 university teachers from both public and private universities in Lahore, Pakistan including Riphah International University, University of Education, University of Management and Technology, and the University of Punjab, were recruited over a six-month period from January 1, 2022, to June 30, 2022. The initial sample size of 377 was calculated using the Raosoft online calculator with a 95% confidence level, a 5% margin of error, and a 50% response distribution. However, 15 incomplete datasets were excluded, leaving a final sample of 362 for analysis.
Participants included university teachers aged 25 to 60 years who consented to participate. Caffeine users were defined as those consuming at least five cups of caffeinated beverages (e.g., tea, green tea, or coffee) daily and working for a minimum of eight hours per day. Teachers consuming fewer caffeinated drinks were categorized as non-caffeine users. Teachers with pre-existing voice disorders due to laryngeal or neurological pathologies (such as vocal nodules, tumors, recurrent laryngeal nerve palsy) or those diagnosed with hypo- or hyperthyroidism were excluded from the study.
Ethical approval was obtained from the Research & Ethical Committee (REC) of Riphah College of Rehabilitation and Allied Health Sciences, Riphah International University, Lahore (Ref No. REC/RCR & AHS/22/0615, dated December 29, 2021). Informed consent was secured from all participating teachers, and the aims and objectives of the study were clearly communicated to them. Participant confidentiality was strictly maintained. Data were collected using a basic demographic sheet and the Voice Handicap Index (VHI). 11 The VHI, a validated 30-item self-assessment tool, evaluates voice handicap across three subscales: Functional, Emotional, and Physical. Participants were asked to complete the VHI questionnaire.
Data were analyzed using SPSS version 22.0. Descriptive statistics, including frequencies and percentages, were calculated for demographic variables. The chi-square test was used to determine the distribution of categorical variables related to caffeine consumption. The means of VHI total and subscale scores were calculated, and independent t-tests were employed to assess differences between the caffeine and non-caffeine user groups, accounting for variance. Multivariate analysis was conducted to explore correlations between demographic variables and caffeine consumption with respect to VHI scores and subscales. Statistical significance was set at p<0.05.
RESULTS
The study sample consisted of 362 university teachers, with a predominance of females (n=239, 66%). A significant portion of participants (n=92, 25.4%) fell within the 30-35 years’ age group. The majority of the teachers (n=290 out of 362) were identified as caffeine users (Table 1). Additionally, a large proportion (192, 54.1%) reported experiencing severe voice handicaps (Figure 1).
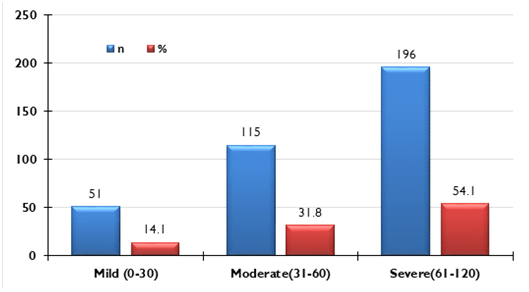
Figure 1: Distribution of Severity of Voice handicap index among sample population (n=362)
More males (113 out of 123) were caffeine users while only 177 out of 239 females were caffeine users and the difference was significant (p<0.001). Age association also revealed that most of those >45 years of age were noncaffeine users compared to age groups of 25-40 in which all were caffeine users (p<0.001). 196(54.1%) had severe voice handicaps out of which 72 (19.9%) were noncaffeine users, while in the category of mild and moderate handicaps, all were caffeine users (p<0.001) (Table I).
Table I: Association between caffeine use and demographic variables with voice handicap severity among university teachers
|
Variable |
Group |
Frequency (%) (n=362) |
Caffeine Use |
Chi-square |
||
|
Yes (n=290) |
No (n=72) |
X2 |
p-value |
|||
|
Gender |
Males |
123 (34) |
113 |
10 |
16.169 |
<0.001 |
|
Females |
239 (66) |
177 |
62 |
|||
|
Age (years) |
25-30 |
85 (23.5) |
85 |
0 |
265.113 |
<0.001 |
|
30-35 |
92 (25.4) |
92 |
0 |
|||
|
35-40 |
75 (20.7) |
75 |
0 |
|||
|
40-45 |
64 (17.7) |
38 |
26 |
|||
|
>45 |
46 (12.7) |
0 |
46 |
|||
|
Severity |
Mild (0-30) |
51 (14.1) |
51 |
0 |
76.119 |
<0.001 |
|
Moderate (31-60) |
115 (31.8) |
115 |
0 |
|||
|
Severe (61-120) |
196 (54.1) |
124 |
72 |
|||
T-test analysis demonstrated that the VHI total mean scores, along with the subscale scores for functional, physical, and emotional components, were significantly higher among non-caffeine users compared to caffeine users (p<0.001) [Table II].
Table II: Comparison of Voice handicap index total and subscale scores between caffeine users and Non-Users (n=362)
|
Scale |
Subscale |
Caffeine Use |
||
|
Caffeine User (n=290) |
Non User (n=72) |
t-test |
||
|
Mean±SD |
Mean±SD |
t, p-value |
||
|
Voice handicap index |
Functional |
15.68±4.19 |
18.97±2.06 |
-6.474, <0.001 |
|
Physical |
16.33±9.38 |
33.50±1.99 |
-15.436, <0.001 |
|
|
Emotional |
21.36±9.77 |
33.64±2.22 |
-10.589, <0.001 |
|
|
Total |
53.37±20.36 |
86.11±3.63 |
-13.582, <0.001 |
|
The correlation between age, gender, and VHI scale and subscale scores (Table III) revealed a significant association between gender and caffeine use (p<0.001). Males had significantly higher total VHI, functional subscale, and mean scores compared to females (p<0.001). In the physical domain, female caffeine users exhibited higher mean scores, while male non-caffeine users showed higher mean scores. In the emotional domain, male caffeine users had higher mean scores, whereas female non-caffeine users displayed higher scores.
Table III: Correlation Between Gender, Age, and voice Handicap Index Scale and Subscale Scores Among Caffeine Users and non-Users
|
Variable |
VHI Scale & Subscale |
Group |
Caffeine User |
|
|
|
Yes |
No |
Variable* User Correlation |
|||
|
Mean±SD |
Mean±SD |
F,P-value |
|||
|
Gender |
Functional |
Males |
14.81±5.28 |
21.80±1.03 |
86.51, <0.001 |
|
Females |
16.23±3.22 |
18.52±1.80 |
|||
|
Physical |
Males |
16.19±10.03 |
33.80±1.40 |
217.64, <0.001 |
|
|
Females |
16.42±8.97 |
33.45±2.07 |
|||
|
Emotional |
Males |
29.56±2.51 |
32.50±1.96 |
850.92, <0.001 |
|
|
Females |
16.13±9.05 |
33.82±2.22 |
|||
|
Total |
Males |
60.55±16.95 |
88.10±4.18 |
487.16, <0.001 |
|
|
Females |
48.78±21.05 |
85.79±3.47 |
|||
|
Age (years) |
Functional |
25-30 |
12.39±3.57 |
|
199.11, <0.001 |
|
30-35 |
15.66±4.48 |
|
|||
|
35-40 |
17.28±2.12 |
|
|||
|
40-45 |
19.89±1.33 |
19.73±1.80 |
|||
|
>45 |
|
18.54±2.08 |
|||
|
Physical |
25-30 |
11.79±7.30 |
|
376.03, <0.001 |
|
|
30-35 |
13.67±10.87 |
|
|||
|
35-40 |
18.80±5.33 |
|
|||
|
40-45 |
28.03±0.97 |
31.46±1.39 |
|||
|
>45 |
|
34.65±1.18 |
|||
|
Emotional |
25-30 |
29.22±2.72 |
|
405.05, <0.001 |
|
|
30-35 |
13.76±11.36 |
|
|||
|
35-40 |
18.17±5.08 |
|
|||
|
40-45 |
28.47±1.11 |
31.58±1.63 |
|||
|
>45 |
|
34.80±1.57 |
|||
|
Total |
25-30 |
53.40±13.13 |
|
498.95, <0.001 |
|
|
30-35 |
43.10±26.50 |
|
|||
|
35-40 |
54.25±12.31 |
|
|||
|
40-45 |
76.39±2.64 |
82.77±2.49 |
|||
|
>45 |
|
88.00±2.70 |
|||
The correlation between age and caffeine use was also significant (p<0.001), with non-caffeine users in the higher age groups showing significantly higher total VHI, physical, and emotional subscale scores. However, for the functional subscale, the highest scores were observed among caffeine users aged 40-45 years, followed closely by non-caffeine users in the same age group.
DISCUSSION
The current study revealed that severe voice handicap was prevalent in 196 participants (54.1%), while only 51 (14.1%) had a mild handicap. Notably, all caffeine users (290, 80.1%) exhibited some degree of voice issues across varying severities. Interestingly, caffeine users had significantly lower VHI scores compared to non-caffeine users (p=0.000). Among those with mild to moderate voice handicaps, all were caffeine users, whereas 124 of the 196 severe cases were caffeine users, and 72 (19.9%) severe cases were non-caffeine users.
In a cross-sectional study by Azari S, et al., 41% of professors reported voice issues, with caffeine use being common. ¹² However, a study by Franca MC et al. found that 30 minutes after ingesting 100 mg of caffeine, there was no significant difference in acoustic and aerodynamic measurements compared to a placebo. ¹³ The severe voice handicaps observed in non-caffeine users in this study may be incidental and related to unreported underlying pathologies, potentially due to a lack of awareness about vocal health.
Regarding the mild to moderate handicaps seen in caffeine users, it is possible that tolerance to the side effects of caffeine may have developed, varying by age and gender. ¹⁴ This could be influenced by individual differences, particularly polymorphism in the CYP1A2 isoform of cytochrome P450, which metabolizes 95% of ingested caffeine. ¹⁵
Byeon, in a study, reported that caffeine was a major risk factor affecting vocal disorders in teachers.¹⁶ Similarly, Akhtar S, et al., found that 250 mg of caffeine caused irregularities in frequencies during free speech, reading, and even singing.¹⁷ Akinbode R, et al., also reported a significant association between dysphonia and regular caffeine consumption.¹⁸ However, in contrast, the current study found that VHI scale and subscale scores for functional, physical, and emotional components, as well as total mean scores, were significantly higher in non-caffeine users (p<0.001). This aligns with studies by Levendoski EE et al.,¹⁹ and Ahmed EE et al.,²⁰ which found no significant effect of caffeine on vocal function in a Saudi Arabian cohort. The protective effect of caffeine, particularly in tea containing a higher amount of milk, common in Asian and Arabian cultures, might explain these differences.
Byeon's study also highlighted age and caffeine consumption as major risk factors for vocal disorders in teachers. ¹⁶ Similarly, in the present study, the majority of those over 45 years old were non-caffeine users, whereas caffeine users were predominantly in the 25–40-year age group (p<0.001). The correlation between age and caffeine use was significant (p<0.001), with higher total VHI, physical, and emotional subscale scores for non-caffeine users in older age groups. Functional subscale scores were highest among caffeine users aged 40-45 years, followed by non-caffeine users. Literature, however, does not consistently show an association between age and VHI scores¹⁸,²⁰ or coffee intake.²⁰ Moy FM, et al., similarly reported no correlation between age and VHI total and subscale scores in a study involving school teachers.²¹
The current study revealed that a higher proportion of males were caffeine users, with 113 out of 123 males consuming caffeine, compared to 177 out of 239 females, and the difference was statistically significant (p<0.001). This finding contrasts with a study by Dillon P, et al., which reported that females had significantly higher caffeine usage than males (p<0.001).²²
In the present study, the correlation between gender and VHI scale and subscale scores showed significant results (p<0.001), indicating that males had significantly higher total VHI and functional subscale mean scores. However, the physical domain showed higher mean scores for female caffeine users, while male non-caffeine users had higher mean scores. In the emotional domain, males who were caffeine users scored higher, whereas females who were non-caffeine users had higher scores. Conversely, Ahmed EE, et al., did not find a significant association between gender and VHI scores (p=0.26),²⁰ and Byeon H, reported that gender was not a major risk factor for vocal disorders in teachers.¹⁶ In contrast, Alarouj H, et al. noted that female teachers had higher VHI scores compared to their male counterparts (p<0.001).²³
The findings of the present study suggest there may be variations in caffeine metabolism among individuals. ¹⁵ In Pakistan, tea and coffee are typically consumed with a significant amount of dairy milk. Research indicates that the polyphenols found in coffee bind to dairy amino acids, enhancing anti-inflammatory effects in mouse cells, suggesting that adding milk to caffeinated beverages like coffee could have anti-inflammatory benefits. ²⁴ This might explain the observed beneficial effects of caffeine among university teachers in the current study.
Limitations of the study
The study was conducted solely in Punjab, which limits the geographic diversity of the sample and may affect the generalizability of the findings to university teachers in other regions of the country. Additionally, the use of a non-probability convenience sampling technique may introduce selection bias, as it relies on a sample that may not accurately represent the broader population of university teachers. This limitation further reduces the generalizability of the study's findings. Moreover, the lack of awareness among teachers regarding voice disorders and voice-related quality of life posed challenges during data collection, potentially affecting the reliability of the self-reported data.
CONCLUSION
The current study concludes that, in the Pakistani context, caffeine does not have a significant impact on voice handicaps, which may be influenced by cultural factors such as the common practice of adding milk to caffeinated drinks. However, gender and age were found to have a significant correlation with voice handicap, suggesting that these demographic factors play a more prominent role in influencing vocal health.
REFERENCES
1. Rodak K, Kokot I, Kratz EM. Caffeine as a factor influencing the functioning of the human body-friend or foe? Nutrients 2021;13(9):3088. https://doi.org/10.3390/nu13093088
2. Bdullahi R, Lawal A, Ibrahim M, Khalid A, Muhammad U. Assessment of the level of caffeine in some tea leaves marketed in dutse: Jigawa state. Korean J Food Health Converg 2019;5(3):7-20. https://doi.org/10.13106/kjfhc.2019.vol5.no3.7
3. Knapik JJ, Steelman RA, Trone DW, Farina EK, Lieberman HR. Prevalence of caffeine consumers, daily caffeine consumption, and factors associated with caffeine use among active duty United States military personnel. Nutr J 2022;21(1):22. https://doi.org/10.1186/s12937-022-00774-0
4. Azari S, Aghaz A, Maarefvand M, Ghelichi L, Pashazadeh F, Shavaki YA. The prevalence of voice disorders and the related factors in university professors: a systematic review and meta-analysis. J Voice 2022:S0892-1997(22)00057-1. https://doi.org/10.1016/j.jvoice.2022.02.017
5. Franca MC, Simpson KO, Schuette A. Effects of caffeine on vocal acoustic and aerodynamic measures of adult females. CoDAS 2013;25(3):250-5. https://doi.org/10.1590/s2317-17822013000300010
6. Kahlenberg RD, Potter H. Why teacher voice matters. American Educator. Winter 2014-15. [Accessed on: July 10, 2023]. Available from URL:https://www.aft.org/sites/default/files/kahlenberg.pdf
7. Mahmoud NF, Khaled DMF. Mohammed HO. Knowledge of Egyptian faculty members about voice care: a national cross-sectional study. Egypt J Otolaryngol 2022;38:59. https://doi.org/10.1186/s43163-022-00247-5
8. Kyriakou K, Petinou K, Phinikettos I. Risk factors for voice disorders in university professors in cyprus. J Voice 2018;32(5): 643.e1-643.e9. https://doi.org/10.1016/j.jvoice.2017.07.005
9. Georgalas VL, Kalantzi N, Harpur I, Kenny C. The effects of caffeine on voice: a systematic review. J Voice. 2023;37(4):636.e7-636.e19. https://doi.org/10.1016/j.jvoice.2021.02.025
10. Bolbol SA, Zalat MM, Hammam RA, Elnakeb NL. Risk factors of voice disorders and impact of vocal hygiene awareness program among teachers in public schools in Egypt. J Voice 2017;31(2):251e.9-251e.16. https://doi.org/10.1016/j.jvoice.2016.07.010
11. Johnson AF, Jacobson B, Grywalski C, Silbergleit A, Jacobson G, Benninger MS. The Voice Handicap Index (VHI). Am J Speech Lang Pathol 1997;6(3):66-70. https://doi.org/10.1044/1058-0360.0603.66
12. Grandjean AC, Reimers KJ, Bannick KE, Haven MC. The effect of caffeinated, non-caffeinated, caloric and non-caloric beverages on hydration. J Am Coll Nutr 2000;19(5):591-600. https://doi.org/10.1080/07315724.2000.10718956.
13. Nehlig A. Interindividual differences in caffeine metabolism and factors driving caffeine consumption. Pharmacological Rev 2018;70(2):384-411. https://doi.org/10.1124/pr.117.014407
14. Byeon H. The risk factors related to voice disorder in teachers: a systematic review and meta-analysis. Int J Environ Res Public Health 2019;16(19):3675. https://doi.org/10.3390/ijerph16193675.
15. Akhtar S, Wood G, Rubin JS, O'Flynn PE, Ratcliffe P. Effect of caffeine on the vocal folds: a pilot study. J Laryngol Otol 1999;113(4):341-5. https://doi.org/10.1017/s0022215100143920
16. Akinbode R, Lam KBH, Ayres JG, Sadhra S. Voice disorders in Nigerian primary school teachers. Occup Med 2014;64:382–86. https://doi.org/10.1093/occmed/kqu052
17. Levendoski EE, Sivasankar S. Investigating the effects of caffeine on phonation. J Voice 2011;25(5):215-9. https://doi.org/10.1016/j.jvoice.2011.02.009
18. Ahmed EE, Bukhari MA, Melibary RA. Voice disorders among academic staff at king saud university medical college (comparison between basic science and clinical staff). J Otolaryngol ENT Res 2017;8(1):394‒6. https://doi.org/10.15406/joentr.2017.08.00233
19. Moy FM, Hoe VCW, Hairi NN, Chu AHY, Bulgiba A, Koh D. Determinants and effects of voice disorders among secondary school teachers in Peninsular Malaysia using a validated malay version of VHI-10. PLoS One 2015;10(11):e0141963. https://doi.org/10.1371/journal.pone.0141963
20. Dillon P, Kelpin S, Kendler K, Thacker L, Dick D, Svikis D. Gender differences in any-source caffeine and energy drink use and associated adverse health behaviors. J Caffeine Adenosine Res 2019;9(1):12–9. https://doi.org/10.1089/caff.2018.0008
21. Alarouj H, Althekerallah JM, AlAli H, Ebrahim MA. A comparative study utilizing the Voice Handicap Index-10 (VHI-10) in teachers and the general population of Kuwait. J Voice 2022;36(2):289.e1-299.e10. https://doi.org/10.1016/j.jvoice.2020.05.006
22. Flynn H. Can adding milk to a cup of coffee have anti-inflammatory effects? Medical News. [Accessed on: July 3, 2023]. Available from URL: https://www.medicalnewstoday.com/articles/can-adding-milk-to-a-cup-of-coffee-have-anti-inflammatory-effects
Following authors have made substantial contributions to the manuscript as under:
MBB: Acquisition of data, analysis and interpretation of data, drafting the manuscript, approval of the final version to be published NM & GM: Conception and study design, analysis and interpretation of data, critical review, approval of the final version to be published
Authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST Authors declared no conflict of interest, whether financial or otherwise, that could influence the integrity, objectivity, or validity of their research work.
GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |