![]() https://doi.org/10.35845/kmuj.2024.23340 ORIGINAL ARTICLE
https://doi.org/10.35845/kmuj.2024.23340 ORIGINAL ARTICLE
Oral Health-Related Quality of Life in patients receiving fixed orthodontic treatment
Aneela
Nausheen![]() 1
2, Sheraz Fazid
1
2, Sheraz Fazid![]() 1,
Umar Hussain
1,
Umar Hussain![]() 3,Zia
Ul Haq
3,Zia
Ul Haq![]() 1
1
|
1: Institute of Public Health & Social Sciences, Khyber Medical University, Peshawar, Pakistan 2: Department of Orthodontics, Rehman College of Dentistry, Peshawar, Pakistan 3: Department of Orthodontics, Saidu College of Dentistry, Swat, Pakistan
Email
Contact #: +92-300-1064455
Date Submitted: March 07, 2023 Date Revised: June 07, 2024 Date Accepted: June 09, 2024 |
|
THIS ARTICLE MAY BE CITED AS: Nausheen A, Fazid S, Hussain U, Haq ZU. Oral Health-Related Quality of Life in patients receiving fixed orthodontic treatment. Khyber Med Univ J 2024;16 (2):134-9. https://doi.org/10.35845/kmuj.2024.23340 |
ABSTRACT
OBJECTIVE: To determine Oral Health Related Quality of Life (OHRQoL) in patients receiving fixed orthodontic treatment
METHODS: This study was conducted at department of Orthodontics, Khyber College of Dentistry, Peshawar from 24th March 2022 to 30th June 2022. One hundred and seventy-five patients, undergoing fixed orthodontic therapy for at least three months were included in the study. Patients with oral diseases that directly or indirectly affect OHRQoL, any previous orthodontic treatment, cognitive impairment and craniofacial anomalies were excluded. The OHRQoL was recorded using Oral Health Impact Profile-14 (OHIP-14) questionnaire. Independent samples t-test was used to examine the relationship between age and gender with total OHIP-14 score. Comparison of OHIP-14 score among socioeconomic levels and educational level was done using one way ANOVA.
RESULTS: The mean age of the participants was 23.13±5.25 years, OHIP-14 score was 29.48±7.36 and 56% (n=98) were females. No significant difference was found between gender, age of the participants, socioeconomic status (SES) and the OHIP-14 score (p=0.05). Highest mean OHIP-14 score was found in ‘higher educational level’ followed by intermediate then secondary school and least in primary education level and it was very highly statistically significant (ANOVA test, p<0.001). Participants had negative effect on pronouncing words (47%), physical pain (88%), and psychological discomfort and social disability (94%).
CONCLUSION: Fixed orthodontic appliances significantly impact participants' QoL, with educational level varying, while gender, age, and SES showed no significant effect on OHIP-14 scores. Functional limitations, physical pain, psychological discomfort, and social challenges were prominent domains affected by orthodontic treatment.
KEYWORDS: Oral Health (MeSH); Quality of Life (MeSH); Psychological Well-Being (MeSH); Orthodontic Appliances, Fixed (MeSH); Orthodontic Brackets (MeSH); Public Health Dentistry (MeSH); Dental Health Surveys (MeSH).
INTRODUCTION
Oral and dento-facial issues impact not only physical health but also psychological well-being and quality of life (QoL)1, with malocclusion being a significant dental concern.2,3Aesthetic concerns and associated psychosocial challenges are prominent issues related to malocclusion.3 Correcting malocclusion leads to improved facial aesthetics and increased self-esteem.4
Fixed orthodontic treatment is a standard approach for correcting various types of malocclusions.5The primary reasons motivating individuals to seek orthodontic treatment are its social and psychological impacts.6 Besides correcting malocclusions, perceived benefits include enhancements in dental and facial aesthetics, as well as improvements in social well-being and psychological confidence.6-9
Health-related quality of life (HRQoL) instruments assess both physical and mental health status and their impact on overall QoL.10HRQoL is typically evaluated using self-report methods such as questionnaires.11Oral Health-Related Quality of Life (OHRQoL) is defined as the absence of negative impacts of oral conditions on social life and a positive sense of dento-facial self-confidence.12 The Oral Health Impact Profile (OHIP) serves as a subjective measure of OHRQoL, offering multidimensional insights into the physical and psychosocial effects of oral conditions on individuals' well-being.
Originally developed by Slade and Spencer in 1994, the Oral Health Impact Profile-49 (OHIP-49) consists of 49 questions.13 Subsequently, Slade introduced a shorter version in 1997 known as Oral Health Impact Profile-14 (OHIP-14). This abbreviated version comprises14 questions covering seven domains: functional limitation, physical discomfort, psychological discomfort, physical disability, psychological disability, social disability, and handicaps.
Feu et al.,14 conducted a study on 284 subjects aged 12 to 15 years undergoing fixed appliance therapy, using OHIP-14 to assess quality of life before treatment, after one year, and at two years. Their findings indicated that while fixed appliance treatment initially negatively impacted quality of life, it improved significantly after treatment completion.
Enhancing OHRQoL is a universal goal for patients, including those undergoing orthodontic treatment with fixed appliances. These appliances can temporarily affect social interactions, speech, and chewing abilities during active treatment phases. However, there is limited local literature on this topic. This study was planned to quantify OHRQoL in patients undergoing fixed appliance treatment at the Orthodontic department of Khyber College of Dentistry, Peshawar-Pakistan. With various orthodontic appliances available, orthodontists can choose alternatives to address poor OHRQoL when necessary.
METHODS
This descriptive cross-sectional study was conducted at the Orthodontic department of Khyber College of Dentistry Peshawar, in collaboration with Institute of Public Health & Social Sciences, Khyber Medical University, Peshawar, Pakistan, spanning from March 24, 2022, to June 30, 2022. Sample size calculation was performed using Open Epi software, based on a previous study by Machale P,15 reporting an 86.92% prevalence of overall impact of fixed appliances on OHRQoL. The desired margin of error was set at 5% with a 95% confidence interval, resulting in an estimated sample size of 175 participants.
Participants were selected using non-probability consecutive sampling criteria: individuals undergoing fixed orthodontic therapy for a minimum of three months. Participants with oral diseases (broken/missing teeth, periodontal diseases, caries, and oral soft tissue infections) that could potentially cause cognitive impairment and/or psychological problems, as well as those with craniofacial anomalies/syndromes were excluded from the study.
Ethical approval for this study was granted by the Ethical Review Committee of Khyber Medical University under reference KMU/IPHSS/Ethics/2023/EO/095 and approved from advanced study board of Khyber Medical University Peshawar for Master in Health research via reference number DIR/KMU-AS&RB/EF/001658,dated April11, 2022.
The study protocol was thoroughly explained to all participants, and written informed consent was obtained from each individual.
All patients who had fixed orthodontic appliances placed at the Orthodontic department of Khyber College of Dentistry, Peshawar, Pakistan, were invited to complete a structured proforma. This proforma captured socio-demographic details, including socioeconomic status16, age, gender, and education level, along with an OHIP-14 questionnaire. Data collection occurred during participants' routine orthodontic visits.
The OHIP-14 questionnaire assessed patients' OHRQoL through responses rated on a 5-point Likert scale: 0=Never, 1=Rarely, 2=Sometimes, 3=Often, 4=Daily. Responses were categorized to indicate whether OHRQoL was affected: "no effect" (responses 0 and 1) or "effect present" (responses 2, 3, and 4).
Statistical analysis was conducted using SPSS version 22.0. Descriptive statistics were computed to summarize the data. The independent sample t-test was employed to compare OHIP-14 scores across different age groups and genders. Additionally, one-way ANOVA was utilized to compare OHIP-14 scores among different socioeconomic levels and educational levels.
The Shapiro-Wilk test was used to assess the normality of the data, and it indicated that the data were normally distributed (p = 0.217). A significance level (p-value) of 0.05 was predetermined to determine statistical significance.
RESULTS
The mean age of the participants was 23.13±5.25 years with range from 15 to 35 years The mean OHIP-14 score was 29.48±7.36. Females comprised the majority, with 98 participants (56%), outnumbering males, who totaled 77 (44%). The age group with the highest representation was 'more than 20 years', accounting for 122 participants (70%). Among participants, 76 (43%) were classified as having a low income level, followed by 75 (43%) categorized as medium income. The most common educational attainment was intermediate, with 73 (42%) subjects (Table I).
Table I: Demographic Characteristics of Study Participants
|
Variable |
Characteristic |
Frequency (Percentage) (n= 175) |
|
Gender |
Female |
98 (56) |
|
Male |
77 (44) |
|
|
Age group (years) |
≤20 |
53 (30) |
|
>20 |
122 (70) |
|
|
Socio-economic status |
High |
24 (14) |
|
Low |
76 (43) |
|
|
Middle |
75 (43) |
|
|
Educational level |
Higher (graduate and post graduate) |
46 (26) |
|
Intermediate |
73 (42) |
|
|
Matric |
27 (15) |
|
|
Primary |
29 (17) |
Functional limitations in the OHIP-14 questionnaire revealed that 83 participants (47%) experienced difficulty pronouncing words, while 162 (93%) reported a worsened sense of taste. In the physical pain category, 154 participants (88%) found eating uncomfortable, and 118 (67%) expressed concerns about self-consciousness. Psychological discomfort was noted in 165 participants (94%) feeling tense and 163 (93%) dissatisfied with their diet. Regarding physical disability, 128 participants (73%) experienced meal interruptions, and 130 (74%) found it difficult to relax. In the psychological disability category, 146 participants (83%) felt embarrassed, and 165 (94%) reported irritability with others. Social disability affected 165 participants (94%), who had ‘difficulty doing their usual jobs’. For handicap category of OHIP-14 about 118 (67%) had ‘feeling that life in general was less satisfying’ and 133 (76%) were ‘totally unable to function’ (Table II).
Table II: Distribution of Responses in Oral Health Impact Profile-14 (OHIP-14) Questionnaire Domains
|
Domain |
Question |
Characteristics |
Frequency (Percentage) (n= 175) |
|
Functional limitation |
Trouble pronouncing any words |
Effect present |
83 (47) |
|
No effect |
92 (53) |
||
|
Worsened sense of taste |
Effect present |
162 (93) |
|
|
No effect |
13 (7.4) |
||
|
Physical pain |
Uncomfortable to eat any foods |
Effect present |
154 (88) |
|
No effect |
21 (12) |
||
|
Worried or self-conscious |
Effect present |
118 (67) |
|
|
No effect |
57 (33) |
||
|
Psychological discomfort |
Felt tense |
Effect present |
165 (94) |
|
No effect |
10 (5.7) |
||
|
Diet been unsatisfactory |
Effect present |
163 (93) |
|
|
No effect |
12 (6.9) |
||
|
Physical disability |
Interrupt meals |
Effect present |
128 (73) |
|
No effect |
47 (27) |
||
|
Difficult to relax |
Effect present |
130 (74) |
|
|
No effect |
45 (26) |
||
|
Psychological disability |
Bit embarrassed |
Effect present |
146 (83) |
|
No effect |
29 (17) |
||
|
Bit irritable with other people |
Effect present |
165 (94) |
|
|
No effect |
10 (5.7) |
||
|
Social disability |
Difficulty doing your usual jobs |
Effect present |
165 (94) |
|
No effect |
10 (5.7) |
||
|
Handicap |
Felt that life in general was less satisfying |
Effect present |
118 (67) |
|
No effect |
57 (33) |
||
|
Totally unable to function |
Effect present |
133 (76) |
|
|
No effect |
42 (24) |
The mean OHIP-14 score was similar in females (29.84 ±7.67) and males (29.03±6.97) and results were statistically non-significant (p=0.466). Similarly, among age groups the mean difference in OHIP-14 score (mean diff= -0.12) was not significant statistically (p=0.921) [Table III].
Table III: OHIP-14 Scores Stratified by Gender and Age Group among Patients with Fixed Appliances
|
Variable |
Characteristic |
OHIP-14 ScoresMean(SD) |
Difference |
95% CI |
p-value* |
|
Gender |
Male |
29.03 (6.97) |
0.81 |
-1.4, 3.0 |
0.466 |
|
Female |
29.84 (7.67) |
||||
|
Age group (years) |
≤20 |
29.40 (7.32) |
-0.12 |
-2.5, 2.3 |
0.921 |
|
>20 |
29.52 (7.41) |
*student t-test, OHIP-14: Oral Health Impact Profile-14
The mean of OHIP-14 score among various socioeconomic levels was almost similar. The difference in mean was also not statistically significant (ANOVA test p-value=0.51), [Figure 1].
![]()
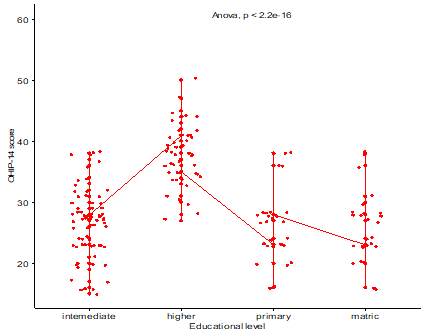
The line graph illustrates that the highest mean OHIP-14 score was observed among participants with higher educational levels, followed by those with intermediate and secondary (matric) education, and the lowest among those with primary education. A one-way ANOVA test indicated highly significant statistical differences (p < 0.001) [Figure 2].
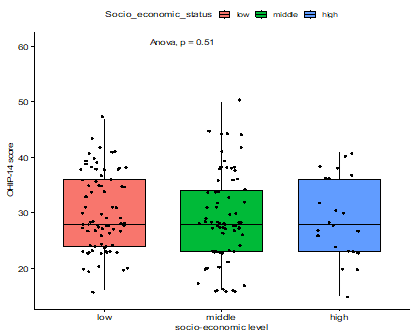
Figure 2: Oral Health Impact Profile-14 (OHIP-14) score stratified by educational levels
DISCUSSION
This study was conducted to determine OHRQoL in patients receiving fixed orthodontic treatment. Our findings showed that fixed orthodontic treatment is associated with poor OHRQoL. Gender and educational level emerged as significant factors influencing OHRQoL during this treatment.
The participants had a mean age of 23.13±5.25 years, a period when individuals, particularly teenagers and young adults, are often most concerned about their dental appearance due to malocclusion. This age range is typical for undergoing orthodontic treatment, consistent with findings from previous studies that also highlight the impact of fixed appliances on OHRQoL among individuals of similar ages.17,18
In our study sample, females constituted 56%, outnumbering males who accounted for 44%. This higher proportion of females can be attributed to their heightened awareness and concern regarding facial esthetics compared to males. Similar findings have been reported in previous studies. For instance, Chen et al.19 conducted research in China on the impact of fixed appliance therapy on OHRQoL, where females comprised 66.6% of the sample, while males accounted for 33.3%. Similarly, a study from Saudi Arabia examining the effect of fixed appliances on OHRQoL reported 69% females and 31% males.20
Our findings showed that speech, chewing and social engagement is negatively affected among patients wearing fixed appliances. Similar results were found in the previous literature.20-22The mean OHIP-14 score was similar in females (29.84±7.67) and males (29.03±6.97) and was statistically non-significant (p=0.466). A previous study in Saudi Arabia by Baidas et al also reported that the difference in mean OHIP-14 score among genders was not statistically significant (p=0.701).20 Another study also reported non-significant difference for OHIP-14 score among gender.22However, some authors found that statistical difference exist among gender for OHI-14 score.21 The variations among thefindings can be attributed to ethnic and genetic factors and also to variations in the methodologies of research.
The current study showed no significant association of age with OHIP-14 score (p=0.921). A previous study conducted in Malaysia on orthodontic patients also reported that mean OHIP-14 score was not different among adolescent and young patients (p=0.691).23 However, study by Baidaset al.20 reported that mean OHIP-14 score was higher in adults (14.85±13.32) than adolescent (4.72±6.46) and it was statistically significant (p=0.007).
Our findings revealed that individuals with higher educational levels exhibited the highest mean OHIP-14 scores, followed by those with intermediate and secondary education, and the lowest scores were observed among those with primary education (p < 0.001). A previous study similarly reported higher mean OHIP-14 scores in college compared to high school, though the difference was not statistically significant (16.73±14.64 vs. 9.69±10.90, p = 0.073).24
There was no statistically significant difference observed in the mean OHIP-14 scores between females and males, indicating that gender did not exert a significant influence on OHRQoL scores. However, Females in our study demonstrated greater concern and self-consciousness compared to males, affecting their QOL. This aligns with previous studies that have also highlighted a more pronounced negative effect of orthodontic treatment on females compared to males.22,25 McGrath et al.25 further supported this observation, suggesting that females' heightened sensitivity and ability to articulate their feelings and perceptions may contribute to this disparity.
Limitations of the study
This study had several limitations. We did not investigate the relationship between various types and severity of malocclusion and their impact on OHRQoL. Additionally, the absence of a comparison group limits our ability to accurately determine the true effect of fixed orthodontic treatment. Future research should consider randomized designs to better assess the genuine impact of fixed orthodontic treatment on OHRQoL.
CONCLUSION
Fixed orthodontic appliances have a significant impact on participants' quality of life. While gender, age, and socioeconomic status did not influence OHIP-14 scores significantly, educational level showed distinct variations. Functional limitations, physical pain, psychological discomfort, and social challenges were prominent domains affected by orthodontic treatment.
REFERENCES
1. Gift HC, Redford M. Oral health and the quality of life. Clin Geriatric Med 1992;8(3):673-84.
2. Bedi R, Gulati N, McGrath C. A study of satisfaction with dental services among adults in the United Kingdom. Br Dent J 2005;198(7):433-7.https://doi.org/10.1038/sj.bdj.4812198
3. Borzabadi-Farahani A, Borzabadi-Farahani A. Agreement between the index of complexity, outcome, and need and the dental and aesthetic components of the index of orthodontic treatment need. Am J Orthod Dentofacial Orthop 2011;140:233-8.https://doi.org/10.1016/j.ajodo.2010.09.028
4. Badran SA. The effect of malocclusion and self-perceived aesthetics on the self-esteem of a sample of Jordanian adolescents. Eur J Orthod 2010;32(6):638-44.https://doi.org/10.1093/ejo/cjq014
6. de Oliveira CM, Sheiham A. Orthodontic treatment and its impact on oral health-related quality of life in Brazilian adolescents. J Orthod 2004;31(1):20-7.https://doi.org/10.1179/146531204225011364.
7. Prabakaran R, Seymour S, Moles DR, Cunningham SJ. Motivation for orthodontic treatment investigated with Q-methodology: patients’ and parents’ perspectives. Am J Orthod Dentofacial Orthop2012;142(2):213-20.https://doi.org/10.1016/j.ajodo.2012.03.026
8. Phillips C, Broder HL, Bennett ME. Dentofacial disharmony: motivations for seeking treatment. Int J Adult Orthodon Orthognath Surg 1997;12(1):7.
9. Kenealy PM, Kingdon A, Richmond S, Shaw WC. The Cardiff dental study: a 20-year critical evaluation of the psychological health gain from orthodontic treatment. Br J Health Psychol 2007;12:17-49.https://doi.org//10.1348/135910706X96896
10. Revicki DA, Kleinman L, Cella D. A history of health-related quality of life outcomes in psychiatry. Dialogues Clin Neurosci 2014;16:127-35.https://doi.org/10.31887/DCNS.2014.16.2/drevicki
11. Hays RD, Reeve BB. Measurement and modeling of health-related quality of life. Int Encyclopedia Public Health 2008:241-52.https://doi.org/10.1016/B978-012373960-5.00336-1
12. Liu Z, McGrath C, Hagg U. The impact of malocclusion/orthodontic treatment need on the quality of life:asystematic review. Angle Orthod 2009;79:585-91.https://doi.org/10.2319/042108-224.1
14. Feu D, Miguel JAM, Celeste RK, Oliveira BH. Effect of orthodontic treatment on oral health–related quality of life. Angle Orthod 2013;83(5):892-8. https://doi.org/10.2319/100412-781.1
15. Machale P , Hegde-Shetiya S, Shirahatti R , Agarwal D. Oral Health Related Quality of Life (OHRQoL) amongst Patients Wearing Fixed Orthodontic Appliance in Pimpri, Pune, India - A Cross Sectional Study. Pesqui Bras Odontopediatria Clin Integr 2012;12(3):351-6.
16. Subohi A. Defining income groups. Dawn. 20 November 2006. Accessed on: May 25, 2022. Available from URL:https://www.dawn.com/news/219652/defining-income-groups
17. Johal A, Fleming P, Al Jawad F. A prospective longitudinal controlled assessment of pain experience and oral health-related quality of life in adolescents undergoing fixed appliance treatment. Orthod Craniofac Res 2014;17(3):178-86.https://doi.org/10.1111/ocr.12044
19. Chen M, Wang DW, Wu LP. Fixed orthodontic appliance therapy and its impact on oral health-related quality of life in Chinese patients. Angle Orthod 2010;80(1):49-53.https://doi.org/10.2319/010509-9.1
20. Baidas LF, AlJunaydil N, Demyati M, Sheryei RA. Fixed orthodontic appliance impact on oral health-related quality of life during initial stages of treatment. Niger J Clin Pract 2020;23(9):1207-14.https://doi.org/10.4103/njcp.njcp_681_19
21. Mansor N, Saub R, Othman SA. Changes in the oral health-related quality of life 24 h following insertion of fixed orthodontic appliances. J Orthod Sci 2012;1(4):98.https://doi.org/10.4103/2278-0203.105880
22. Scheurer PA, Firestone AR, Burgin WB. Perception of pain as a result of orthodontic treatment with fixed appliances. Eur J Orthod 1996;18:34957.https://doi.org/10.1093/ejo/18.4.349
23. Broder HL, Wilson-Genderson M, Sischo L. Examination of a theoretical model for oral health–related quality of life among youths with cleft. Am J Public Health2014;104(5):865-71.https://doi.org/10.2105/AJPH.2013.301686
24. Feu D, Miguel JAM, Celeste RK, Oliveira BH. Effect of orthodontic treatment on oral health–related quality of life. Angle Orthod 2013;83(5):892-8.https://doi.org/10.2319/100412-781.1
25. Kvam E, Gjerdet N, Bondevik O. Traumatic ulcers and pain during orthodontic treatment. Community Dent Oral Epidemiol 1987;15:104-7.https://doi.org/10.1111/j.1600-0528.1987.tb00493.x
|
CONFLICT OF INTEREST Authors declared no conflict of interest, whether financial or otherwise, that could influence the integrity, objectivity, or validity of their research work. GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |