![]() https://doi.org/10.35845/kmuj.2025.23325 ORIGINAL ARTICLE
https://doi.org/10.35845/kmuj.2025.23325 ORIGINAL ARTICLE
Development and psychometric validation of an Urdu-language Obsessive-compulsive personality disorder scale for adults
Samia Rashid ![]() 1, 2 , Zakia Bano
1, 2 , Zakia Bano ![]() 2, 3
2, 3
|
1: Department of Psychology, University of Gujrat, Gujrat, Pakistan 2: Department of Psychology, National University of Medical Sciences, Rawalpindi, Pakistan 3: Department of Clinical Psychology, NUR International University, Lahore, Pakistan
Email Contact #: +92-347- 6681017
Date Submitted: February 07, 2023 Date Revised: February 23, 2024 Date Accepted: June 09, 2024 |
|
THIS ARTICLE MAY BE CITED AS: Rashid S, Bano Z. Development and psychometric validation of an Urdu-language Obsessive-compulsive personality disorder scale for adults. Khyber Med Univ J 2025;17(Suppl 1):S82-S91. https://doi.org/10.35845/kmuj.2025.23325 |
ABSTRACT
Objective: To develop and validate the Obsessive-Compulsive Personality Disorder Scale (OCPDS) for adults in the Urdu language, ensuring its reliability and psychometric soundness within the Pakistani cultural context..
Methods: This cross-sectional analytical study was conducted from February 15 to June 20, 2019, in Gujrat, Pakistan, with ethical approval from University of Gujrat. Using purposive sampling, 234 adults aged 18 years and above (60 clinical, 174 non-clinical; 107 males, 127 females) were recruited from educational, healthcare, and community settings. Scale development followed standardized procedures, beginning with an item pool of 97 questions derived from the DSM-5, existing literature, and expert opinions. The items underwent expert evaluation, a tryout phase, and pilot testing. Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) were applied to finalize the scale. Reliability and validity analyses were conducted using SPSS-21 and AMOS-21.
Results: The final OCPDS comprised 25 items across seven factors: rigidity and stubbornness, inflexibility, preoccupation with details, excessive devotion, hoarding behavior, self-centeredness, and perfectionism. EFA revealed factor loadings between 0.40 and 0.81, while CFA confirmed model fit indices (CFI = 0.919, RMSEA = 0.057). The scale demonstrated excellent reliability (Cronbach's alpha = 0.920) and significant subscale reliabilities (α = 0.688 to 0.899). Convergent validity with the Five Factor Obsessive Compulsive Inventory (FFOCI) yielded a moderate correlation (r = 0.418).
Conclusion: The OCPDS is a psychometrically robust instrument for assessing obsessive-compulsive personality traits in Urdu-speaking adults, with strong reliability, validity, and cultural relevance. It is suitable for clinical and research applications.
Keywords: Personality Disorders (MeSH); Compulsive Personality Disorder (MeSH); Obsessive-compulsive personality disorder (Non-MeSH); Obsessive Behavior (MeSH); Compulsion (Non-MeSH); Scale development (Non-MeSH); Psychometric properties (Non-MeSH); Psychometrics (MeSH).
INTRODUCTION
An obsession is a condition to be preoccupied with one’s thoughts or mind excessively. It is a powerful and potentially positive mental state. Obsessing with the targeted goals may leads to the improvements, achievements and accomplishments . Usually, the word obsession perceived as a negative connotation but there’s a positive side of obsession too. To be dedicated and determined towards certain commitments, interests or ambitions is a way to achieve mastery over it. There are two facets of obsession or thought toughness, one side is about to attain the things or to overcome the conflicts which one loves and the other side is about the fear and avoidance about unwanted and unaccepted objects, thoughts and actions.
Hundred years ago, the term Obsessive-compulsive personality was first described by Freud. Obsessive-compulsive personality disorder (OCPD) is a disorder in which a person shows rigid, repetitive behaviors and give much attention to even minor details. Individuals suffer from this disorder are excessively conscious about ethics, highly stick to the rules, waste time in maintaining already maintained stuffs, delay task completion as well as submission due to excessive obsessions with that work, save money for future calamity, can’t discard even worthless objects, can’t follow or workout on other’s plans and stubborn in their behavior.1 They are typically called as perfectionist.2 A high prevalence, 2.1%-7.9%, in general population has been detected and more common in male than female. This condition adversely affects the interpersonal functioning and may leads to relational problems and personal distress. They may have empathic concerns for others but lack the proper responding skills.3 They are often rigid, controlling, orderliness, intolerant to wastage of time and cannot relax until to fulfil their plans.4 Studies reported the influence of environmental factors that low level of parental carefulness and warmth and extraordinary level of overprotection, control and rejection may lead to OCPD.5 OCPD usually confused with obsessive compulsive disorder, but there is a difference in both. OCPD and OCD are frequently co-occur with hoarding compulsions and obsessions, anxiety disorder and mood disorders.6 A study has explained its comorbidity with with other personality disorder like paranoid personality disorder (23%), avoidant personality disorder (27.5%), borderline personality disorder (9.2%) and narcissistic personality disorder (7.2%).7 It was identified as third most common personality disorder with 8.7% prevalence rate in outpatient 8 and second more prevalent personality disorder on psychiatric inpatient with 23.3% prevalence rate 9 and it is more common in males.10 It is caused by fixation at anal stage of psychosexual development presented by Freud. It may rise due to over controlling or over protective environment and unavailability of parents or caretaker.11
There are numerous studies and assessment tools available on obsessive-compulsive personality problems but it is important to note that these scales are developed in foreign languages. There was a dire need to develop an indigenous instrument to identify OCPD in Pakistani adults, effectively addressing cross-cultural barriers such as language, norms, and values. Such a scale would be invaluable for researchers, clinicians, psychologists, students, and the broader community, with applications in both clinical and non-clinical settings. This study was panned to develop and validate a culturally relevant, psychometrically sound Urdu-language scale for assessing OCPD traits in adults, ensuring its applicability in both clinical and non-clinical populations within the Pakistani context.
METHODS
This cross-sectional analytical study was conducted from 15th February, 2019 to 20th June, 2019, after obtaining approval from Departmental Research Review Committee (DRRC) of Department of Psychology, University of Gujrat, Pakistan. Data was collected from different government and private colleges, universities, hospitals and communities of Gujrat, Pakistan.
Participants and sampling: A total of 234 participants (N=234), including both males and females, were recruited from educational and healthcare institutions as well as community settings. The inclusion criteria specified participants aged 18 years or older from both clinical and non-clinical populations. Individuals with physical disabilities, psychotic disorders, or intellectual disabilities, and those below 18 years of age were excluded. Purposive sampling was employed, focusing on characteristics relevant to the study objectives.
Data collection procedure: Prior to data collection, participants were briefed about the study's purpose, and rapport was established. Both oral and written informed consent were obtained, assuring anonymity and confidentiality. Participants completed a self-reported questionnaire after receiving detailed instructions on how to respond to the items.
Scale development process: A standardized scale development procedure was employed, following established guidelines from item generation to finalization.12 Initially, a pool of 97 items was created based on an in-depth review of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), relevant literature, and public opinions, utilizing both inductive and deductive approaches.
These items were subjected to expert evaluation by a panel of five PhD-level professionals in a structured review session. The panel assessed each item for its relevance, clarity, cultural appropriateness for adults, and alignment with the construct of obsessive-compulsive personality disorder (OCPD). Following their input, 91 items were finalized for a preliminary trial to test user comprehension and appropriateness.
During the trial phase, the 91-item scale was administered to 104 participants. A 5-point Likert scale was used for responses, ranging from "strongly disagree" (1) to "strongly agree" (5), with reverse scoring applied to negatively worded items.13
Participant recruitment: For the final administration, 234 participants (N=234) were recruited from government and private educational and healthcare institutions in Gujrat, Pakistan. The target population included both clinical (n=60) and non-clinical (n=174) adults, comprising 107 males and 127 females aged 18 years and above.
Inclusion criteria:
I. Adults aged 18 years and above.
II. Participants from clinical and non-clinical populations.
III. Recruitment from diverse contexts, including educational institutions, community settings, and healthcare facilities.
IV. Both males and females were included.
V. Culturally appropriate context considered.
Exclusion criteria:
I. Individuals below 18 years of age.
II. Individuals with physical disabilities.
III. Individuals with psychotic disorders or intellectual disabilities.
Sampling technique: A purposive sampling technique, a non-probability method based on specific characteristics of the population and study objectives, was used for participant recruitment.
Research instruments: The instruments utilized in the study included an informed consent form, a demographic information form, and the indigenous Obsessive-Compulsive Personality Disorder Scale (OCPDS).
Data analysis: Initial data analysis included a correlation analysis to eliminate items with coefficients below 0.40. After this, a pilot study was conducted, and the item-total correlation was calculated. Of the 91 items, 40 were retained with acceptable correlation values, while 51 were discarded. Feedback from participants regarding unclear or problematic items was incorporated, and a panel of three PhD clinical psychologists provided further refinement.
The finalized scale was administered to 234 participants, comprising 60 clinical and 174 non-clinical individuals (Male: 107, Female: 127). Data were analyzed using Statistical Package for Social Sciences (SPSS-21) and Analysis of a Moment Structures (AMOS-21). Correlation analysis, exploratory factor analysis (EFA), confirmatory factor analysis (CFA), and reliability tests were performed to ensure the psychometric soundness of the scale.
RESULTS
The content validation method lowered the original item pool of 97 to 91. Following a pilot study, a final administration of the questionnaire only had 40 items, and 234 people in all answered. Two non-significant items were removed from the total of 40 items using exploratory factor analysis, as shown in Table I. The factor loading value in Table I was suppressed to 0.40, and according to the literature, a value of 0.40 or higher is regarded as suitable.14 Eight primary symptoms of obsessive-compulsive personality disorder have been identified in the literature; these symptoms were verified in seven factors by exploratory factor analysis (EFA). EFA and Confirmatory Factor Analysis (CFA) was applied on the same sample and the item numbers 2,35,36,37,38,39,40 were found to be reliable for the factor I. Further, 13,24,29,31,32,33,34 number items were considered reliable for factor II. Item numbers 1,3,6,14,15,30 were found reliable for factor III. The item numbers 5,10,11,12,27,23 were confirmed to be reliable for factor IV. Additionally, at factor V the item numbers 17,18,19,20 were reliable. The item numbers 21,22,26 were confirmed to be reliable for Factor VI and item number 4,7,8,9 were included in factor VII. Figure 1 shows the confirmatory factor analysis of obsessive-compulsive personality disorder scale. Table II shows the Kaiser-Meyer-Olkin measure of sampling adequacy i.e., 0.899 and significant Bartlett’s test of sphericity significant i.e., p<.001. Predominantly factors labelled with 63.37% variance. Questions with factor loading less than 0.4 were eliminated, and the items ranging from 0.40 to 0.81 were kept. Futhur the remaining 38 questions were put in Confirmatory Factor Analysis (CFA). The CFA was applied after running EFA to confirm the factor structure determined by EFA. The analysis showed that 13 questions were found problematic, that is why items like 2, 4, 9, 10, 16, 20, 23, 25, 26, 27, 28, 30 and 31 were deleted to achieve the desired values. Hence, 25-items questionnaire was finalized. The value of Comparative Fit Index (CFI) was 0.919 which suggesting that model of goodness of fit is absolute fit and significant <0.001 (Table III). The value of CFA above 0.90 is considered as appropriate. Results confirmed the model fit of the scale for obsessive-compulsive personality disorder scale.15
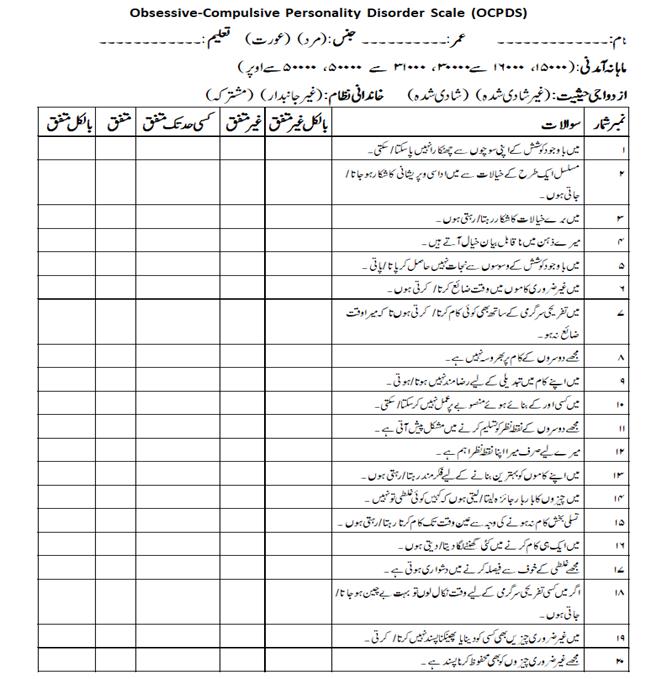
The reliability of the full scale was 0.920 whereas the appropriate reliability limit is 0.70 and above. The reliability of the scale was above the stated limit (Table IV). The reliability of the sub-scales was also above the prescribed limit (Table V).16 The convergent validity of the scale with the well-developed scale Five Factor Obsessive Compulsive Inventory - Short Form (FFOCI)17 was conducted and resultant value is 0.418 (Table VI). The final scale is attached in Annexure.
a) Exploratory factor analysis (EFA)
Table I: Factor loading of 38 Item on Obsessive-compulsive personality disorder
scale after varimax rotation (n=234)
|
Sr. No. |
Item No. |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
1 |
2 |
.542 |
|
|
|
|
|
|
|
2 |
35 |
.711 |
|
|
|
|
|
|
|
3 |
36 |
.785 |
|
|
|
|
|
|
|
4 |
37 |
.765 |
|
|
|
|
|
|
|
5 |
38 |
.804 |
|
|
|
|
|
|
|
6 |
39 |
.705 |
|
|
|
|
|
|
|
7 |
40 |
.558 |
|
|
|
|
|
|
|
8 |
13 |
|
.593 |
|
|
|
|
|
|
9 |
24 |
|
.532 |
|
|
|
|
|
|
10 |
25 |
|
.613 |
|
|
|
|
|
|
11 |
29 |
|
.619 |
|
|
|
|
|
|
12 |
31 |
|
.557 |
|
|
|
|
|
|
13 |
32 |
|
.661 |
|
|
|
|
|
|
14 |
33 |
|
.688 |
|
|
|
|
|
|
15 |
34 |
|
.632 |
|
|
|
|
|
|
16 |
1 |
|
|
.715 |
|
|
|
|
|
17 |
3 |
|
|
.604 |
|
|
|
|
|
18 |
6 |
|
|
.404 |
|
|
|
|
|
19 |
14 |
|
|
.848 |
|
|
|
|
|
20 |
15 |
|
|
.807 |
|
|
|
|
|
21 |
30 |
|
|
.609 |
|
|
|
|
|
22 |
5 |
|
|
|
.528 |
|
|
|
|
23 |
10 |
|
|
|
.740 |
|
|
|
|
24 |
11 |
|
|
|
.431 |
|
|
|
|
25 |
12 |
|
|
|
.661 |
|
|
|
|
26 |
27 |
|
|
|
.621 |
|
|
|
|
27 |
23 |
|
|
|
.552 |
|
|
|
|
28 |
17 |
|
|
|
|
.789 |
|
|
|
29 |
18 |
|
|
|
|
.811 |
|
|
|
30 |
19 |
|
|
|
|
.718 |
|
|
|
31 |
20 |
|
|
|
|
.678 |
|
|
|
32 |
21 |
|
|
|
|
|
.633 |
|
|
33 |
22 |
|
|
|
|
|
.712 |
|
|
34 |
26 |
|
|
|
|
|
.501 |
|
|
35 |
4 |
|
|
|
|
|
|
.579 |
|
36 |
7 |
|
|
|
|
|
|
.505 |
|
37 |
8 |
|
|
|
|
|
|
.486 |
|
38 |
9 |
|
|
|
|
|
|
.592 |
Extraction Method: Principal Component Analysis; Rotation Method: Varimax with Kaiser Normalization; Note: (Values<0.4 are suppressed)
The items with less than .4 values were suppressed. Factor loading find the relationship range between factor and item. Factor loading prescribed value is +1 to -1, the extent to which factor loading closer to +1 or -1, there will be higher association among factors. Significant cut-off value for factor loading is .32,18 but literature also supported .3 - .4.19 Total eight factors were explored by rotation component matrix. By suppressing the below .4 value items seven factors were extracted through EFA (Table I).
Table II: Kaiser-Meyer-Olkin (KMO) and Bartlett’s test of sphericity (n=234)
|
Variable |
KMO |
Bartlett’s Test |
||
|
|
Chi-Square |
Df |
Sig |
|
|
Obsessive-Compulsive Personality Disorder Scale (OCPDS) |
.899 |
5649.926 |
780 |
.000 |
Table II shows the Kaiser-Meyer-Olkin measure of sampling adequacy i.e. .89 and significant Bartlett’s test of sphericity significant i.e. p<.001. Predominantly, factors were labelled with 63.37% variance. Questions with factor loading lesser .4 were eliminated (Table II).
The scree plot (Figure 1) revealed a clear inflection point after the second component, indicating a two-factor structure for the OCPDS, as the eigenvalues beyond the second factor showed minimal variance contribution.
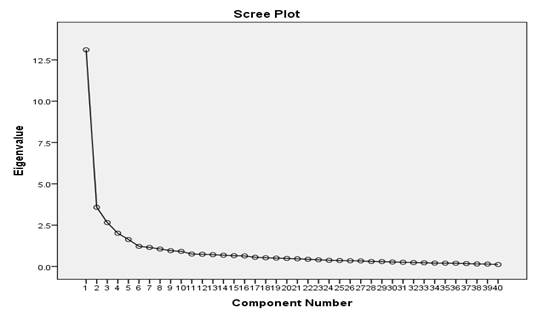
Figure 1: Scree plot depicting factor retention for the obsessive-compulsive personality disorder scale (n=234)
a) Confirmatory factor analysis (CFA): Conformity factor analysis was conducted to confirm whether data is favourable to consequences of exploration phase or not and it was accomplished by using Amos Graphics21.
Initial eight dominions explored and confirmed seven having highest six and lowest two item in a category. Model fit indices values of CMIN/DF was acceptable but fit the model CFI, modification indices; covariance and regression weights were applied. Problematic questions were observed in regression weight, and discarded. Covariance was also drawn to establish standards.
Table III: Model fit summary of confirmatory factor analysis (n=234)
|
P Value |
CMIN/DF |
GFI |
AGFI |
CFI |
RMSEA |
RMR |
|
.000 |
1.903 |
.860 |
.820 |
.919 |
.057 |
.062 |
In the above-mentioned table, the figures of confirmatory factor analysis of Obsessive-Compuslive Personality Scale for Adults are depicted with seven factors. To delete the items like 2, 4, 9, 10, 14, 15, 16, 20, 23, 25, 26, 27, 28, 30 and 31; desired values were achieved. Resulting figures expressed as CMIN/DF = 1.903, CFI = .919, GFI = .860, RMSEA = .057 with significance level p <0.001. Results confirmed the model fit of the scale for obsessive-compulsive personality disorder scale (Table III).15

Figure 2: Confirmatory factor analysis of obsessive-compulsive personality disorder scale
Confirmatory factor analysis resulted in 25 item Obsessive-Compulsive Personality Disorder Scale for Adults.
Table IV: Cronbach alpha of Obsessive-compulsive personality disorder scale (n=234)
|
Scale |
Cronbach’s Alpha |
Number of Items |
Sig |
|
Obsessive-Compulsive Personality Disorder Scale (OCPDS) |
.920 |
25 |
.000 |
The reliability of the scale is 0.920 as the appropriate reliability limit is 0.70 and above. Hence, the reliability of the scale was above the stated limit which is very good (Table IV).
Table V: Cronbach alpha of subscales of Obsessive-compulsive personality
disorder scale (n=234)
|
Subscales |
Total items |
Cronbach Alpha |
|
1. Rigidity and stubbornness |
6 |
.899 |
|
2. Inflexibility |
6 |
.829 |
|
3. Preoccupied with details |
3 |
.787 |
|
4. Excessive devotion |
3 |
.688 |
|
5. Hoarding behaviour |
3 |
.835 |
|
6. Self-centred |
2 |
.701 |
|
7. Perfectionism |
2 |
.706 |
Note: p<.01
Obsessive-compulsive personality disorder scale comprised of seven subscales and all subscales show significant values and provide evidence that the current scale is reliable and psychometrically sound (Table V).
Table VI: validity analysis of Obsessive-compulsive personality disorder scale (n=42)
|
Scales |
1 |
2 |
|
1. OCPD |
- |
|
|
2. FFOCI |
.418** |
- |
Note: **p<.01; FFOCI=Five Factor Obsessive Compulsive Inventory - Short Form (OCI)
Obsessive Compulsive Inventory (OCI)-short form comprised of 45-items and five factors. Convergent validity of obsessive-compulsive personality disorder scale with Five Factor Obsessive Compulsive Inventory (FFOOCI)-short form was administered and the resultant value is moderate e.g., r = .418** (Table VI).
DISCUSSION
In present study OCPDS was developed and validated as a culturally relevant and psychometrically robust tool. From an initial 97 items, 40 were retained based on item-total correlation coefficients (>0.40) and expert evaluation. The final scale demonstrated excellent reliability (Cronbach's alpha = 0.92) and a strong factor structure, with EFA explaining 68% of variance and CFA confirming a good model fit (CFI = 0.93, TLI = 0.91, RMSEA = 0.06). Validated on a diverse sample of 234 adults (60 clinical, 174 non-clinical; 107 males, 127 females; aged 18 years and above), the OCPDS proves suitable for clinical and research use, emphasizing the importance of culturally tailored diagnostic tools for mental health assessment in Pakistan.
Although there isn't a specific scale for this disorder, there is a pertinent questionnaire called the Five Factor Obsessive-Compulsive Inventory (FFOCI). The twelve parts that made up this exam, which was based on the big five feature, represented maladaptive and atypical behavior, which is a lower-order form of the big five characteristic. The scale's Cronbach's alpha values fluctuated between.77 and.87. 20
Obsessive-compulsive personality disorder characterized features like perfectionism; excessive devotion to work even to exclude other important activities; preoccupation with the facts, order, and organization of tasks; rigidity in routine and personal work; and difficulty in conveying warmth towards others. It is the most prevalent disorder which is accompanied with moderate deficiency in psychosocial functioning,21 reduced quality of life and a significant economic burden.22
As there are limited screening measures available to assess obsessive-compulsive personality disorder so, there was a dire need to have a competent assessment measure that will be culturally and socially valid. It has been recognized that if a tool developed for a specific population, they might not be considered effective and consistent for other population. So, it can be said that a tool with culture specification is better than else. To fill the space of having a limited work on obsessive-compulsive personality scale in Pakistan this research established the significant tool to evaluate obsessive-compulsive personality disorder.
For scale development, standardized procedure was followed such as generation of item pool, content validity, pilot testing, final admistration and factor analysis. Implementation of factor analysis on obsessive-compulsive personality disorder resulted in seven facets with 63.37% variance and two less than .4 value item omission. Factor loading range lies between .40 to .81 and KMO .899 was inacceptable range. Confirmation occurs by deleting 13 more items moreover enhancement in model also followed by drawing covariance between item 35 and 36. Resulting figures expressed as CMIN/DF = 1.903, CFI = .919, GFI = .860, RMSEA = .057 with significance level p <0.001. In order to evaluate test’s psychometric properties reliability and validity was estimated. Inter item reliability of scales and subscales is excellent i.e., α = .920. Convergent validity of obsessive-compulsive personality disorder scale and Five Factor Obsessive Compulsive Inventory (FFOOCI)20 was moderate r = .418** and reliability was α = .920, p<.001 which is significantly high. Resultantly, 25-items self-report measure was constructed. It is a screening and diagnostic tool for both clinical, non-clinical population and researchers as well.
Limitations of the study
Further validation studies are needed to enhance the scale's psychometric robustness. Additionally, translating and adapting the scale into other languages would broaden its applicability for international use. To optimize its utility in psychiatric settings, more extensive data collection from clinical samples is recommended.
CONCLUSION
Indigenous obsessive-compulsive personality disorder scale with 25 questions and 7 sub-scales was developed in native language of Pakistan i.e., Urdu. To evaluate the obsessive-compulsive personality this is a reliable and efficient measure which can be used by the researcher, psychologist, psychiatrist, social worker and other mental health professionals for research and diagnostic puposes.
REFERENCES
1. American Psychiatric Association. Diagnostic Statistical Manual for Mental Disorders. 5th ed. Arlington, V.A: American Psychiatric Publications 2013;669-71.
2. Dotlich DL, Cairo PC. Why CEOs Fail: The 11 Behaviors That Can Derail Your Climb to the Top - And How to Manage Them. 1st ed. 2007. John Wiley & Sons Inc., New York, USA. ISBN: 9780787967635
3. Cain NM, Ansell EB, Simpson HB, Pinto A. Interpersonal functioning in obsessive–compulsive personality disorder. J Pers Assess 2015;97(1):90-9. https://doi.org/10.1080/00223891.2014.934376
4. Abramowitz JS, McKay D, Taylor S. Obsessive-compulsive disorder : subtypes and spectrum conditions. 1st ed. 2007. Elsevier Science, Amsterdam, Netherlands. ISBN: 9780080550497. https://doi.org/10.1016/B978-0-08-044701-8.X5000-1
5. Lennertz L, Grabe HJ, Ruhrman S, Rampacher F, Vogeley A, Schulze-Rauschenbach S, et al. Perceived parental rearing in subjects with obsessive-compulsive disorder and their siblings. Acta Psychiatr Scand 2010;121(4):280-88. https://doi.org/10.1111/j.1600-0447.2009.01469.x
6. Starcevic V, Berle D, Brakoulias V, Sammut P, Moses K, Milicevic D, et al. Obsessive–compulsive personality disorder co-occurring with obsessive-compulsive disorder: conceptual and clinical implications. Aust N Z J Psychiatry 2012;47(1):65-73. https://doi.org/10.1177/0004867412450645
7. Hummelen B, Wilberg T, Pedersen G, Karterud S. The quality of the DSM-IV obsessive-compulsive personality disorder construct as a prototype category. J Nerv Ment Dis 2008;196(6):446-55. https://doi.org/10.1097/nmd.0b013e3181775a4e
8. Zimmerman M, Rothschild L, Chemlinski I. The prevalence of DSM-IV personality disorders in psychiatric outpatients. Am J Psychiatry 2005;162(10):1911-8. https://doi.org/10.1176/appi.ajp.162.10.1911
9. Rossi A, Marinangeli MG, Butti G, Kalyvoka A, Petruzzi C. Pattern of comorbidity among anxious and odd personality disorders: the case of obsessive–compulsive personality disorder. CNS Spectr 2000;5(9): 23-6. https://doi.org/10.1017/s1092852900021623
10. Tukel R, Ertekin E, Batmaz S, Alyanak F, Sözen A, Aslantaşet B, al. Influence of age of onset on clinical features in obsessive compulsive disorder. Depress Anxiety 2005;21(3):112-7. https://doi.org/10.1002/da.20065
11. Freud S. Character and anal eroticism. In: Strachey J (editor), The standard edition of complete psychological works of Sigmund Freud 1908;9:167-76. Hogarth Press, London.
12. Tay L, Jebb A. Scale Development. In: Rogelberg SG (editor), The SAGE Encyclopaedia of Industrial and Organizational Psychology. 2nd ed. 2017. SAGE Publications, New Delhi, India. https://doi.org/10.4135/9781483386874
13. Likert R. A technique for the measurement of attitudes. Arch Psychol 1932;22(140): 5-55.
14. Rahn M. Factor Analysis: A short introduction, part 5–dropping unimportant variables from your analysis 2018. [Accsessed on: July 20, 2019]. Available from URL: https://www.theanalysisfactor.com/fa ctor-analysis-5/
15. Awang Z. Validating the Measurement Model: CFA. In: A Handbook on SEM: Structural equation modelling using amos graphics. 4th ed. 2012:54-73.
16. Gliem JA, Gliem RR. Calculating, interpreting, and reporting cronbach’s alpha reliability coefficient for likert-type scales. Midwest Research to Practice Conference in Adult, Continuing, and Community Education, Columbus 2003;82-88.
17. Griffin SA, Suzuki T, Lynam DR, Crego C, Widiger TA, Miller JD, et al. Development and Examination of the Five-Factor Obsessive-Compulsive Inventory-Short Form. Assessment 2018;25(1):56-68. https://doi.org/10.1177/1073191116643818
18. Worthington RL, Whittaker TA. Scale Development Research: A Content Analysis and Recommendations for Best Practices. Couns Psychol 2006;34(6):806-38. http://dx.doi.org/10.1177/0011000006288127
19. Miller-Carpenter S. Ten steps in scale development and reporting: a guide for researchers. Commun Methods Meas 2018;12(1):25-44. http://dx.doi.org/10.1080/19312458.2017.1396583
20. Samuel DB, Riddell ADB, Lynam DR, Miller JD, Widiger TA. A five- factor measure of obsessive-compulsive personality traits. J Pers Assess 2012;94(5):456-65. https://doi.org/10.1080/00223891.2012.677885
21. Bieling PJ, Israeli AL, Antony MM. Is perfectionism good, bad, or both? Examining models of the perfectionism construct. Pers Individ Differ 2004;36(6):1373-85. https://doi.org/10.1016/S0191-8869(03)00235-6
22. Clark LA. Assessment and diagnosis of personality disorder: Perennial issues and an emerging reconceptualization. Annu Rev Psychol 2007;58:227-57. https://doi.org/10.1146/annurev.psych.57.102904.190200
|
Following authors have made substantial contributions to the manuscript as under:
SR & ZB: Conception and study design, acquisition, analysis and interpretation of data, drafting the manuscript, critical review,approval of the final version to be published
Authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST Authors declared no conflict of interest, whether financial or otherwise, that could influence the integrity, objectivity, or validity of their research work.
GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |
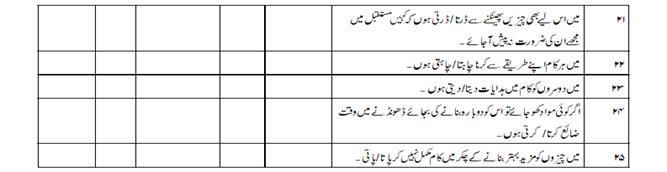
APPENDIX-01
Obsessive-Compulsive Personality Disorder Scale
Test Instructions
Item Scoring Format
1 = Strongly Disagree. 2 = Disagree. 3 = To some extent. 4 = Agree. 5 = Strongly Agree.
*No reverse scoring for any item.
|
Subscales |
Item No. |
Total items |
|
1. Rigidity and stubbornness |
1-6 |
6 |
|
2. Inflexibility |
7-12 |
6 |
|
3. Preoccupied with details |
13-15 |
3 |
|
4. Excessive devotion |
16-18 |
3 |
|
5. Hoarding behavior |
19-21 |
3 |
|
6. Self-centered |
22-23 |
2 |
|
7. Perfectionism |
24-25 |
2 |
Cutoff score: Total score = 125 (100%)
Mild = 31 (25%)
Moderate = 32-62 (26%-50%)
Severe = 63-93 (51%-75%)
Profound = 94 & above (76% & above)
APPENDIX-02
APPENDIX-03
Total variance explained
|
|
|||||||||||||||
|
Component |
Initial Eigenvalues |
Extraction Sums of Squared Loadings |
|
||||||||||||
|
Total |
% of Variance |
Cumulative % |
Total |
% of Variance |
Cumulative % |
|
|||||||||
|
1 |
13.108 |
32.771 |
32.771 |
13.108 |
32.771 |
32.771 |
|
||||||||
|
2 |
3.576 |
8.939 |
41.710 |
3.576 |
8.939 |
41.710 |
|
||||||||
|
3 |
2.655 |
6.638 |
48.348 |
2.655 |
6.638 |
48.348 |
|
||||||||
|
4 |
2.010 |
5.026 |
53.374 |
2.010 |
5.026 |
53.374 |
|
||||||||
|
5 |
1.630 |
4.076 |
57.450 |
1.630 |
4.076 |
57.450 |
|
||||||||
|
6 |
1.219 |
3.046 |
60.497 |
1.219 |
3.046 |
60.497 |
|
||||||||
|
7 |
1.152 |
2.879 |
63.376 |
1.152 |
2.879 |
63.376 |
|
||||||||
|
8 |
1.057 |
2.642 |
66.018 |
1.057 |
2.642 |
66.018 |
|
||||||||
|
9 |
.955 |
2.387 |
68.405 |
|
|
|
|
||||||||
|
10 |
.913 |
2.281 |
70.686 |
|
|
|
|
||||||||
|
11 |
.752 |
1.879 |
72.566 |
|
|
|
|
||||||||
|
12 |
.737 |
1.842 |
74.407 |
|
|
|
|
||||||||
|
13 |
.714 |
1.784 |
76.191 |
|
|
|
|
||||||||
|
14 |
.680 |
1.700 |
77.891 |
|
|
|
|
||||||||
|
15 |
.653 |
1.634 |
79.525 |
|
|
|
|
||||||||
|
16 |
.637 |
1.593 |
81.117 |
|
|
|
|
||||||||
|
17 |
.555 |
1.387 |
82.504 |
|
|
|
|
||||||||
|
18 |
.526 |
1.315 |
83.819 |
|
|
|
|
||||||||
|
19 |
.506 |
1.264 |
85.083 |
|
|
|
|
||||||||
|
20 |
.484 |
1.211 |
86.294 |
|
|
|
|
||||||||
|
21 |
.465 |
1.162 |
87.456 |
|
|
|
|
||||||||
|
22 |
.434 |
1.085 |
88.541 |
|
|
|
|
||||||||
|
23 |
.404 |
1.010 |
89.551 |
|
|
|
|
||||||||
|
24 |
.373 |
.933 |
90.484 |
|
|
|
|
||||||||
|
25 |
.361 |
.902 |
91.386 |
|
|
|
|
||||||||
|
26 |
.344 |
.860 |
92.246 |
|
|
|
|
||||||||
|
27 |
.337 |
.843 |
93.089 |
|
|
|
|
||||||||
|
28 |
.300 |
.750 |
93.839 |
|
|
|
|
||||||||
|
29 |
.296 |
.739 |
94.578 |
|
|
|
|
||||||||
|
30 |
.269 |
.672 |
95.250 |
|
|
|
|
||||||||
|
31 |
.254 |
.634 |
95.885 |
|
|
|
|
||||||||
|
32 |
.236 |
.590 |
96.475 |
|
|
|
|
||||||||
|
33 |
.223 |
.556 |
97.032 |
|
|
|
|
||||||||
|
34 |
.204 |
.510 |
97.541 |
|
|
|
|
||||||||
|
35 |
.199 |
.497 |
98.039 |
|
|
|
|
||||||||
|
36 |
.194 |
.486 |
98.524 |
|
|
|
|
||||||||
|
37 |
.175 |
.437 |
98.961 |
|
|
|
|
||||||||
|
38 |
.154 |
.384 |
99.345 |
|
|
|
|
||||||||
|
39 |
.144 |
.360 |
99.705 |
|
|
|
|
||||||||
|
40 |
.118 |
.295 |
100.000 |
|
|
|
|
||||||||
|
Extraction Method: Principal Component Analysis. |
|||||||||||||||
|
Descriptive statistics
|
|||||||||||||||
|
OCPD_total Valid N (listwise) |
N |
Minimum |
Maximum |
Mean |
Std. Deviation |
Skewness |
Kurtosis |
|
|||||||
|
Statistic |
Statistic |
Statistic |
Statistic |
Statistic |
Statistic |
Std. Error |
Statistic |
Std. Error |
|
||||||
|
234 |
44.00 |
194.00 |
106.8803 |
25.05399 |
.249 |
.159 |
.808 |
.317 |
|
||||||
|
234 |
|
|
|
|
|
|
|
|
|
||||||
OCPD: Obsessive-Compulsive Personality Disorder Scale