![]() https://doi.org/10.35845/kmuj.2024.23324 ORIGINAL
ARTICLE
https://doi.org/10.35845/kmuj.2024.23324 ORIGINAL
ARTICLE
Development and validation of aniIndigenous Urdu-language Dependent personality disorder scale for adults
Samia
Rashid ![]() 1,
2,
Zaqia Bano
1,
2,
Zaqia Bano ![]() 2,
3
2,
3
|
1: Department of Psychology, University of Gujrat, Gujrat, Pakistan 2: Department of Psychology, National University of Medical Sciences, Rawalpindi, Pakistan 3: Department of Clinical Psychology, NUR International University, Lahore, Pakistan
Email Contact #: +92-347- 6681017
Date Submitted: February 07, 2023 Date Revised: June 16, 2024 Date Accepted: July 03, 2024 |
|
THIS ARTICLE MAY BE CITED AS: Rashid S, Bano Z. Development and validation of aniIndigenous Urdu-language Dependent personality disorder scale for adults. Khyber Med Univ J 2025;17(Suppl 1):S74-S81. https://doi.org/10.35845/kmuj.2025.23324 |
ABSTRACT
Objective: To develop and validate an indigenous Dependent Personality Disorder Scale (DPDS) for adults, ensuring strong psychometric properties tailored to the cultural context of Pakistan.
Methods: A cross-sectional analytical design was employed, with ethical approval from the Departmental Research Review Committee at the University of Gujrat. Data collection occurred from February to June 2019 in Gujrat, Pakistan. Participants aged 19 and above, from various educational institutions, hospitals, and communities, were recruited using purposive sampling (N=234; 107 males, 127 females). The study involved two phases: scale development and validation. Initially, a pool of 104 items was created based on literature and expert input, reduced to 94 after expert review, and further refined to 52 items through exploratory factor analysis. Confirmatory factor analysis (CFA) validated a final 25-item scale with satisfactory model fit indices (CMIN/DF=2.108, CFI=0.908, RMSEA=0.069). Reliability was assessed using Cronbach's alpha, and construct validity was determined through convergent validity testing against an existing DPDS measure.
Results: The Kaiser-Meyer-Olkin value was 0.938, and Bartlett’s test of sphericity was significant (p < 0.001), supporting factor analysis suitability. Exploratory factor analysis revealed seven factors explaining 64.39% of the variance. The finalized scale demonstrated high internal consistency (α = 0.932). Subscale reliability ranged from 0.684 to 0.866. Convergent validity showed a strong positive correlation (r = 0.712, p < 0.01) with an established DPDS measure.
Conclusion: The 25-item DPDS is a psychometrically robust, reliable, and valid tool for assessing dependent personality disorder in Pakistani adults, with potential applicability in clinical and research settings.
Keywords: Dependent Personality Disorder (MeSH); Personality Assessment (MeSH); Scale development (Non-MeSH); Convergent validity (Non-MeSH); Reliability (Non-MeSH).
INTRODUCTION
In developmental, personality, social, and clinical psychology, "dependency" is a term often used to describe a personality trait associated with both adaptive and maladaptive functioning. Its behavioral manifestations vary considerably. It is important to distinguish between dependency that serves developmental and/or adaptive purposes, such as ensuring a child’s survival and growth, and pathological expressions of dependency, such as dependent personality disorder (DPD), which are characterized by significant distress and impairments. Pathological dependency has been discussed from various theoretical perspectives, with the prevailing view emphasizing a self-perception of helplessness and frailty. These self-representations significantly influence the intrapersonal and interpersonal dynamics of individuals with DPD.¹
Dependent personality disorder is defined by an excessive reliance on others, including a need for advice when making decisions or starting projects, a preference for working with others rather than independently, compliance with immoral demands to avoid abandonment, lack of assertiveness, low self-confidence, and fear of being alone. Individuals with DPD may feel deserted and disheartened when alone, prefer working even with people they dislike, and constantly require support to complete tasks or make decisions. The diagnostic criteria for DPD include eight symptoms, of which at least five must be present for a diagnosis.² Such individuals often exhibit dutiful, dedicated,³ and clinging behaviors.⁴ According to a 2001-2002 survey, the prevalence of DPD is 0.49%, with equal rates in males and females. However, women’s economic dependency and men’s emotional dependency are associated with a higher risk of domestic-partner abuse. Emotional dependency may also hinder the termination of relationships in victimized or maltreated individuals.⁵
Dependent personality disorder was initially introduced as a subtype of passive-aggressive personality in the DSM-I.⁶ It was later revised in DSM-II and labeled as Asthenic Personality Disorder.⁷ In DSM-III, it was categorized under Cluster C, Anxious-Avoidant Personality Disorders, with specific diagnostic criteria.⁸ DSM-5 describes DPD as abnormal clinging behavior toward others in nearly all aspects of life, from routine activities to major decisions, reflecting a persistent need for help, support, and approval from others.
The prevalence of DPD in the general adult population is 0.49%, increasing to 10%-25% among inpatients, up to 47% among outpatients, and an estimated 5%-10% in clinical settings.¹ DPD frequently co-occurs with mood disorders, anxiety disorders (AD), eating disorders, adjustment disorders, and somatization disorders, with comorbidity rates for depression and anxiety disorders ranging from 10% to 20%.⁹ The disorder is more commonly diagnosed in women, with studies indicating a positive correlation between dependency and femininity and an inverse correlation with masculinity. Women are approximately 40% more likely to be diagnosed with DPD than men. Men may underreport dependency, often portraying themselves as autonomous.¹⁰
Both genetic and sociocultural factors contribute to the development of DPD. Genetic factors, such as familial transmission, account for about 30% of cases. Sociocultural factors, including early childhood adversities like parental neglect, physical or emotional abuse, serious illness, poor peer or social support, and interpersonal stress, can lead to diminished autonomy, increased dependency, and low self-confidence.¹¹
Adulthood is a critical developmental stage that introduces significant changes and challenges, often marked by fear and anxiety in individuals with DPD. They tend to engage in stereotypic behaviors, especially in stressful or isolating situations.
While numerous studies and assessment tools exist for measuring dependency-related issues, these instruments are predominantly developed and validated in Western societies. This raises concerns about their applicability and cultural relevance in other populations. Tools developed for specific populations may lack effectiveness and consistency when used elsewhere, highlighting the importance of culturally tailored measures. Given the limited availability of indigenous personality assessment tools in Pakistan, the current research addresses this gap by developing and validating a culturally appropriate scale to assess dependent personality disorder.
The objective of this study was to develop and validate an indigenous DPD scale for adults, ensuring strong psychometric properties tailored to the cultural context of Pakistan
METHODS
The study was approved by the Departmental Research Review Committee of the Psychology Department, University of Gujrat, Pakistan, and ensuring adherence to ethical guidelines. Data collection was conducted from February 15 to June 20, 2019, using a cross-sectional analytical design. Participants were recruited from government and private colleges, universities, hospitals, and communities in Gujrat, Pakistan. Adults aged 19 years and above, both male and female, were eligible, while psychotic patients and individuals under 19 years were excluded.
A purposive sampling technique was employed due to time constraints. Participants were briefed about the study's purpose, affiliation, and confidentiality assurances before providing verbal and written informed consent. Only those who agreed to participate were included. Self-report questionnaires were used for data collection, and respondents were given detailed instructions on completing the forms after reading each item thoroughly.
Phase I: Development of the Dependent personality disorder scale (DPDS): The first phase involved the construction of the DPDS, following standardized scale development protocols.12 An initial pool of 104 items was generated to assess thoughts, feelings, behaviors, interpersonal relationships, and actions related to dependent personality disorder. Subject specialists reviewed the items for relevance, appropriateness for adults, and construct validity, resulting in 94 items for the tryout phase.
The tryout assessed user understanding and identified potential issues with the scale. The 94-item scale was administered to 104 participants using a 5-point Likert scale ranging from "strongly disagree" (1) to "strongly agree" (5), with reverse scoring for negatively worded items. Items with correlation values below 0.4 were discarded.
In the final phase, a sample of 234 adults (212 non-clinical and 22 clinical participants; Male = 107, Female = 127) was drawn from diverse backgrounds, including schools, colleges, universities, hospitals, and the community. Institutional permissions were obtained, and participants provided informed consent before completing the questionnaire and a demographic form. Exploratory and confirmatory factor analyses were performed, resulting in a finalized 25-item DPDS with strong psychometric properties.
Ethical considerations were maintained throughout the research process.
Data analysis: Data were analyzed using Statistical Package for Social Sciences (SPSS-21) and Analysis of Moment Structures (AMOS-21). Analytical methods included correlation analysis, exploratory factor analysis, confirmatory factor analysis, and reliability testing.
RESULTS
Table I: Kaiser-Meyer-Olkin (KMO) and Bartlett’s test of sphericity (n=234)
|
Variable |
KMO |
Bartlett’s Test |
||
|
Chi-Square |
Df |
Sig |
||
|
Dependent Personality Disorder Scale (DPDS) |
.938 |
9401.326 |
1431 |
.000 |
Results evinced that the Kaiser-Meyer-Olkin value is .93 which is above the normally recommended value i.e., .6 13 and Bartlett’s test of sphericity was significant (p<.001) [Table I].
Table II: Factor loading of 52 item on Dependent personality disorder scale after
varimax rotation (n=234)
|
Sr. No. |
Item No. |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
1 |
8 |
.520 |
|
|
|
|
|
|
|
2 |
9 |
.614 |
|
|
|
|
|
|
|
3 |
10 |
.594 |
|
|
|
|
|
|
|
4 |
11 |
.615 |
|
|
|
|
|
|
|
5 |
12 |
.460 |
|
|
|
|
|
|
|
6 |
14 |
.528 |
|
|
|
|
|
|
|
7 |
26 |
.467 |
|
|
|
|
|
|
|
8 |
31 |
.598 |
|
|
|
|
|
|
|
9 |
41 |
.546 |
|
|
|
|
|
|
|
10 |
42 |
-.771 |
|
|
|
|
|
|
|
11 |
44 |
.625 |
|
|
|
|
|
|
|
12 |
45 |
.658 |
|
|
|
|
|
|
|
13 |
46 |
.470 |
|
|
|
|
|
|
|
14 |
38 |
|
.550 |
|
|
|
|
|
|
15 |
39 |
|
.597 |
|
|
|
|
|
|
16 |
40 |
|
.512 |
|
|
|
|
|
|
17 |
43 |
|
.437 |
|
|
|
|
|
|
18 |
47 |
|
.508 |
|
|
|
|
|
|
19 |
48 |
|
.639 |
|
|
|
|
|
|
20 |
49 |
|
.678 |
|
|
|
|
|
|
21 |
50 |
|
.594 |
|
|
|
|
|
|
22 |
51 |
|
.581 |
|
|
|
|
|
|
23 |
52 |
|
.674 |
|
|
|
|
|
|
24 |
53 |
|
.603 |
|
|
|
|
|
|
25 |
1 |
|
|
.467 |
|
|
|
|
|
26 |
15 |
|
|
.484 |
|
|
|
|
|
27 |
16 |
|
|
.552 |
|
|
|
|
|
28 |
17 |
|
|
.672 |
|
|
|
|
|
29 |
19 |
|
|
.638 |
|
|
|
|
|
30 |
21 |
|
|
.597 |
|
|
|
|
|
31 |
22 |
|
|
.572 |
|
|
|
|
|
32 |
23 |
|
|
.474 |
|
|
|
|
|
33 |
24 |
|
|
.690 |
|
|
|
|
|
34 |
27 |
|
|
|
.588 |
|
|
|
|
35 |
28 |
|
|
|
.639 |
|
|
|
|
36 |
29 |
|
|
|
.611 |
|
|
|
|
37 |
30 |
|
|
|
.537 |
|
|
|
|
38 |
32 |
|
|
|
.569 |
|
|
|
|
39 |
33 |
|
|
|
.584 |
|
|
|
|
40 |
34 |
|
|
|
.547 |
|
|
|
|
41 |
2 |
|
|
|
|
.676 |
|
|
|
42 |
3 |
|
|
|
|
.645 |
|
|
|
43 |
4 |
|
|
|
|
.657 |
|
|
|
44 |
7 |
|
|
|
|
.603 |
|
|
|
45 |
5 |
|
|
|
|
|
.500 |
|
|
46 |
6 |
|
|
|
|
|
.623 |
|
|
47 |
18 |
|
|
|
|
|
.479 |
|
|
48 |
20 |
|
|
|
|
|
.684 |
|
|
49 |
54 |
|
|
|
|
|
.491 |
|
|
50 |
36 |
|
|
|
|
|
|
.674 |
|
51 |
37 |
|
|
|
|
|
|
.692 |
Extraction Method: Principal Component Analysis; Rotation Method: Varimax with Kaiser Normalization; Note: (Values<.4 are suppressed)
Exploratory factor analysis (EFA) initially explored 7 factors which designated with 64.39% variance. Questions with factor stuffing, below .4 were abolished, and ranging from .43 to .77. problematic and single item factor were rejected and revealed 7 final factors (Table II).
Table III: Model fit summary of confirmatory factor analysis (n=234)
|
P Value |
CMIN/DF |
GFI |
AGFI |
CFI |
RMSEA |
RMR |
|
.000 |
2.108 |
.854 |
.814 |
.908 |
.069 |
.060 |
CMIN/DF: chi-square minimum/degree of freedom; GFI: Goodness of Fit Index; CFI: Comparative Fit Index, AGFI: Adjusted Goodness of Fit Index; RMSEA: Root Mean Square of Error Approximation
Model fit indices values of CMIN/DF and RMSEA were satisfactory but to better fit the model CFI modification indices of covariance and regression weights were applied. Tricky questions were observed in regression weight, and rejected. Tricky item deletion leads to worthy CFI value establishment. In the above-mentioned table, the figures of confirmatory factor analysis of Dependent Personality Disorder Scale for Adults are depicted with seven subscales. The items that were removed include item number; 1, 3, 5, 7, 8, 9, 10, 12, 13, 15, 17, 18, 22, 25, 28, 29, 30, 34, 35, 38, 39, 40, 41, 43, 45, 46, 50 and 51. 26 items were discarded and final instrument comprised of 25-items with satisfactory values of model i.e., CMIN/DF = 2.108, CFI = .908, and GFI = .854, RMSEA = .069 with significance level p <0.001 well described values fit the model suitably (Table III).
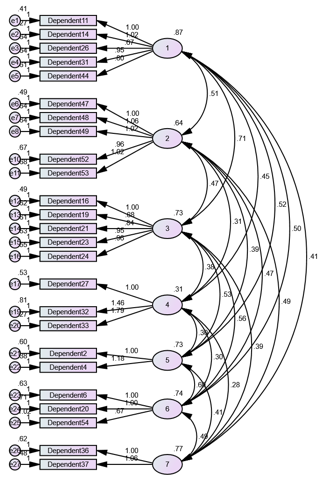
Figure 1: Confirmatory factor analysis of Dependent Personality Disorder Scale
Confirmatory factor analysis resulted in 25 item Dependent Personality Disorder Scale for Adults.
Phase II: Determination of Psychometric Properties of Dependent Personality Disorder Scale
a) Cronbach’s alpha reliability
Table IV: Cronbach alpha of dependent personality disorder scale (n=234)
|
Scale |
Cronbach’s Alpha |
Number of Items |
Sig |
|
Dependent Personality Disorder Scale (DPDS) |
.932 |
26 |
.000 |
|
Cronbach Alpha reliability from 0.70 to 0.90 is considered as moderate to high range. The reliability of the current scale is very good i.e., α = .932 (Table IV).
Table V: Cronbach alpha of subscales of dependent personality disorder scale (n=234) |
|||
|
|
|||
|
Subscales |
Total items |
Cronbach Alpha |
|
1. Need for support |
5 |
.866 |
|
2. Preoccupied with thoughts |
5 |
.842 |
|
3. Need others to assume responsibility |
5 |
.851 |
|
4. Need for care |
3 |
.755 |
|
5. Difficulty in making decision |
2 |
.775 |
|
6. Difficulty in initiating projects or work |
3 |
.684 |
|
7. Difficulty in expressing disagreement |
3 |
.757 |
Note: **p <.01
The reliability of the subscales is also very good which is ranged from .684 to .866. It revealed that the subscale with low reliability value with respect to other subscale is even lie in moderate range (Table V).
b) Construct validity of Dependent personality disorders scale
i) Sample: Sample of 45 (N=45) Male=21, Female=24 recruited from colleges and university faculty and students and community population.
Instrument: To evaluate the convergent validity of newly created Dependent Personality Disorder Scale, Dependent Personality Disorder Scale (DPDS) was used.14 DPDS is a 21-items measure to investigate the excessive clinging and abnormally dependent behaviors.
ii) Results
Table VI: Validity analysis of Dependent personality disorder scale (n= 45)
|
Scales |
1 |
2 |
|
- |
|
|
|
2. DPDS |
.712** |
- |
Note:** p<.01, DPDS = Dependent Personality Disorder Scale
Dependent Personality Disorder Scale (DPDS) was
chosen for convergent validity which reveal good convergent validity with the
new indigenous measure i.e., r=.712**.
Dependent Personality Disorder Scale (English & Urdu versions) are given as Annexures (Appendix 1 & 2).
DISCUSSION
This study successfully developed and validated an indigenous DPDS for adults. EFA identified seven factors explaining 64.39% of the variance, with item loadings of .43–.77. CFA refined the scale to 25 items with strong model fit indices (CMIN/DF = 2.108, CFI = .908, GFI = .854, RMSEA = .069; p < .001). The scale demonstrated excellent reliability (α = .932) and moderate to high subscale reliability (α = .684–.866). Convergent validity was confirmed (r = .712, p < .01), establishing the DPDS as a culturally relevant and psychometrically robust tool for assessing dependent personality traits in Pakistan.
A small percentage of people with DPD are able to lead normal lives, with the majority depending on others to supply their emotional and physical requirements. DPD is a chronic condition. The hallmarks of DPD include extreme worry and terror. Early adulthood is when DPD first manifests, occurs in a range of settings, and is linked to inadequate functioning. Extreme passivity, devastation, or powerlessness once a relationship ends, as well as intense submission and avoidance of duties, can all be symptoms.15
Individuals suffering with dependent personality disorder exhibit an excessive reliance on others for decision-making. They are constantly in need of other people's approval, thus they are unable to make decisions for themselves. As a result, people with DPD frequently prioritize the needs and viewpoints of others over their own since they lack the self-assurance to stand behind their choices. People with DPD often exhibit clinging and passive conduct, which may be explained by this type of behavior. These people exhibit an inability to tolerate solitude and a fear of separation. Because of their intense reliance on others, they feel alone and lonely when they are by themselves.16
DPD is a condition in which a person experiences excessive dependence, excessive disapproval and difficulty in making decisions were core features of dependent personality disorder, presented in DSM-IV which remained same for DSM-IV-R and DSM-5 and categorized in Cluster C personality disorder with two other personality disorder, having the features of fear and anxiety, i.e., avoidant personality disorder and obsessive-compulsive personality disorder. The DSM-5 portrays DPD as abnormal clinging behaviour towards others in every aspect of life from daily living routine to big projects and decisions. They always need help, support and approval form others. This disorder is closely related to anxiety, fear and depression. Individuals need support and guidance in every aspects of their life even in their everyday choices and decisions. Dependent personality disorder is often comorbid with eating disorders, anxiety disorders, and somatization disorders.17
There are few instruments available that dignified Dependent Personality Disorder. There is a questionnaire named Dependent Personality Questionnaire (DPQ) containing eight items and constructed by Tyrer, Morgan, and Cicchetti in 2004.18 The Dependent Personality Inventory (DPI)19 a 55 item questionnaires which is based on DSM-IV TR criteria, seven factor of dependent personality disorders like difficulty in decisions making, accountability, trouble in voicing disagreement, difficulty beginning plans, looking for support from others and feeling alone and abandoned. The Five-Factor Measure of Dependent Traits (FFM DPT) is a twelve-scale measure which presented by Gore and colleagues.20 Although all these measures are well established but these are constructed in Ennglish language and culture bound. Therefore an indigenous measure is established to overcome the language and cultural barrires.
Keenly considering the standardized steps of scale development a scale was developed. Factor determination was executed for dependent personality disorders and outcome reveal seven aspects. 54 items reduced to 51 items segregating in different factors. Result values were observed and made sure before to proceed towards next step that either it would proceed or not. Outcomes showed the KMO is .938, 64.39% variance and factor loaded between .43 to .77 ranges. These values support to move forward for confirmation of factor through second type of factor analysis. Deletion of 26 items reduced to 25 final items with satisfactory values of model i.e., CMIN/DF = 2.108, CFI = .908, and GFI = .854, RMSEA = .069 with significance level p <0.001 well described values fit the model suitably. Dependent Personality Disorder Scale (DPDS)14 was chosen for convergent validity which reveal good correlation r=.712**. Whereas reliability of the test’s scales and subscales was very good i.e., α = .932.
There aren't many screening instruments available to detect dependent personality disorder, thus a capable one that is socially and culturally valid was much needed. It's common knowledge that instruments designed for a particular group of people might not be seen as trustworthy and consistent by other groups. Therefore, a tool with cultural criteria is better than one without. To fill the vacuum left by the dearth of studies on the dependent personality scale in Pakistan, this study created a crucial instrument to evaluate dependent personality disorder.
It is suggested that more validation studies can be carried out to improve its psychometric soundness. In order to be utilized globally, it can also be modified and translated into different languages. To enhance its application in psychiatric settings, more data on clinical samples can be gathered.
CONCLUSION
The development and validation of the Dependent Personality Disorder Scale for adults mark a significant contribution to culturally relevant psychological assessment tools in Pakistan. The scale demonstrated robust psychometric properties, including strong reliability and validity, as evidenced by exploratory and confirmatory factor analyses. The finalized 25-item DPDS, with its seven subscales, effectively captures the multidimensional nature of dependent personality traits and provides a reliable framework for assessing such behaviors in clinical and non-clinical settings. Future studies should explore the scale's applicability in broader populations and examine its predictive and discriminative validity to enhance its utility in diverse clinical and research contexts.
REFERENCES
1. Bornstein RF. Dependent personality disorder. In, Widiger TA (Editor), The Oxford handbook of personality disorders. Oxford University Press 2012:505-26. https://doi.org/10.1093/oxfordhb/9780199735013.013.0023
2. American Psychiatric Association. Diagnostic Statistical Manual for Mental Disorders. 5th ed. American Psychiatric Publications, Arlington, V.A. 2013;669-71.
3. Oldham JM, Morris LD. The New Personality Self-Portrait: Why You Think, Work, Love and Act the Way You Do. 1st ed. 1991. Bantam, New York, USA.
4. Miller L. From Difficult to Disturbed: Understanding and Managing Dysfunctional Employees. 1st ed. 2008. AMACOM, New York, USA.
5. Bornstein RF. The complex relationship between dependency and domestic violence: converging psychological factors and social forces. Am Psychol 2006;61(6):595-606. https://doi.org/10.1037/0003-066x.61.6.595
6. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 1st ed, 1952. American Psychiatric Association, Washington, DC.
7. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 2nd ed, 1968. American Psychiatric Association, Washington, DC.
8. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 3rd ed, 1980. American Psychiatric Association; Arlington, V.A.
9. Beitz K, Bornstein RF. Dependent personality disorder. In, Fisher JE, O'Donahue WT (eds), Practitioner's Guide to Evidence-based Psychotherapy. Springer, New York. 2006;230-37.
10. Tyrka AR, Wyche MC, Kelly MM, Price LH, Carpenter LL. Childhood maltreatment and adult personality disorder symptoms: influence of maltreatment type. Psychiatry Res 2009;165(3):281-7. https://doi.org/10.1016/j.psychres.2007.10.017
11. Amanda KS. The Effect of Sex and Gender Role Orientation on Attitudes towards Individuals with Dependent Personality Disorder (A dissertation). 2012. Indiana State University Terre Haute, Indiana. Accessed on: January 07, 2023. Available from URL: https://scholars.indianastate.edu/etds/1468/
12. Tay L, Jebb A. Scale Development. In: Rogelberg SG (editor), The SAGE Encyclopaedia of Industrial and Organizational Psychology. 2nd ed. 2017. SAGE Publications, New Delhi, India. https://doi.org/10.4135/9781483386874
13. Awang Z. Validating the Measurement Model: CFA. In: A Handbook on SEM: Structural equation modelling using amos graphics. 4th ed. 2012:54-73.
14. Shahzadi A, Bano Z. Development of dependent personality disorder scale: role of nail biting among adults of Sialkot. Khyber Med Uni J 2020;12(4):278-83. https://doi.org/10.35845/kmuj.2020.19802
15. Simonelli A, Parolin M. Dependent personality disorder. Encycl Pers Individ Dif 2017;1-18. http://dx.doi.org/10.1007/978-3-319-28099-8-578-1
16. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed., text rev.).2022. https://doi.org/10.1176/appi.books.9780890425787
17. Bornstein RF. The dependent personality: developmental, social, and clinical perspectives. Psychol Bull 1992;112(1):3-23. https://doi.org/10.1037/0033-2909.112.1.3
18. Tyrer P, Morgan J, Cicchetti D. The dependent personality questionnaire (dpq): a screening instrument for dependent personality. Int J Soc Psychiatry 2004;50(1):10-17. https://doi.org/10.1177/0020764004038754
19. Huber NM. Dependent Personality Inventory (DPI): A Scale to Assess Dependent Personality Subtypes Based on DSM-IV-TR Criteria. Unpublished Master’s Thesis, Cleveland, OH: Cleveland State University. 2005. Accessed on: January 07, 2023. Available from URL: https://engagedscholarship.csuohio.edu/cgi/viewcontent.cgi?article=1600&context=etdarchive
20. Gore WL, Presnall JR, Miller JD, Lynam DR, Widiger TA. A five-factor of dependent personality traits. J Pers Assess 2012;94:488-99. https://doi.org/10.1080/00223891.2012.670681
|
Following authors have made substantial contributions to the manuscript as under:
SR & ZB: Conception and study design, acquisition, analysis and interpretation of data, drafting the manuscript, critical review,approval of the final version to be published
Authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST Authors declared no conflict of interest, whether financial or otherwise, that could influence the integrity, objectivity, or validity of their research work.
GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |
APPENDIX-01
Dependent Personality Disorder Scale
Test Instructions
Item Scoring Format
1 = Strongly Disagree. 2 = Disagree. 3 = To some extent. 4 = Agree. 5 = Strongly Agree.
*No reverse scoring for any item.
|
Subscales |
Item No. |
Total items |
|
1. Need for support |
1-5 |
5 |
|
2. Preoccupied with thoughts |
6-10 |
5 |
|
3. Need others to assume responsibility |
11-15 |
5 |
|
4. Need for care |
16-18 |
3 |
|
5. Difficulty in making decision |
19-20 |
2 |
|
6. Difficulty in initiating projects or work |
21-23 |
3 |
|
7. Difficulty in expressing disagreement |
24-25 |
2 |
APPENDIX-02