![]() https://doi.org/10.35845/kmuj.2025.23322 ORIGINAL ARTICLE
https://doi.org/10.35845/kmuj.2025.23322 ORIGINAL ARTICLE
Development and validation of an indigenous self-rating Narcissistic personality disorder scale for adults in Urdu language
Samia Rashid ![]() 1, 2 , Zaqia Bano
1, 2 , Zaqia Bano ![]() 2, 3
2, 3
|
1: Department of Psychology, University of Gujrat, Gujrat, Pakistan 2: Department of Psychology, National University of Medical Sciences, Rawalpindi, Pakistan 3: Department of Clinical Psychology, NUR International University, Lahore, Pakistan
Email
Contact #: +92-347- 6681017
Date Submitted: February 07, 2023 Date Revised: November 08, 2023 Date Accepted: November 17, 2023 |
|
THIS ARTICLE MAY BE CITED AS: Rashid S, Bano Z. Development and validation of an indigenous self-rating Narcissistic personality disorder scale for adults in Urdu language. Khyber Med Univ J 2025;17(Suppl 1):S54-S63. https://doi.org/10.35845/kmuj.2025.23322 |
ABSTRACT
Objectives: to develop and validate an Urdu-language Narcissistic Personality Disorder (NPD) scale for adults, ensuring robust psychometric properties aligned with Pakistan's cultural context.
Methods: The study was conducted in two phases. In the first phase of the study, a total of 234 participants, aged 19 years and above, were recruited using purposive sampling. The sample included both male and female individuals from clinical and non-clinical populations, drawn from various communities and institutions in Gujrat, Pakistan. An initial pool of 75 items was developed and administered to these participants. Following a systematic scale development process, the final version of the scale was refined to a 25-item self-report questionnaire. In the second phase, the psychometric properties of the scale were evaluated through reliability and validity testing.
Results: Exploratory Factor Analysis (EFA) revealed a nine-factor structure, while Confirmatory Factor Analysis (CFA) refined this to an eight-factor model with an acceptable model fit (CFI=0.926). The scale demonstrated strong psychometric properties, including high internal consistency (α=0.922). The newly developed scale showed significant convergence with the Short Measure of Dark Triads narcissism subscale (r=0.570**). The findings support the scale as a promising diagnostic tool for clinical and research purposes.
Conclusion: Narcissistic Personality Disorder scale is a reliable and valid tool designed to diagnose NPD, overcoming cultural and linguistic barriers by being developed in Urdu. This measure offers utility for researchers and clinicians working in diverse settings.
KEYWORDS: Personality (MeSH); Narcissistic personality (Non-MeSH); Grandiosity (Non-MeSH); Narcissistic Personality Disorder (MeSH); Scale development (Non-MeSH); Convergent validity (Non-MeSH); Reliability (Non-MeSH).
INTRODUCTION
Admiration and recognition are universal desires, but while healthy self-love promotes high self-esteem, excessive self-centeredness can lead to a superiority complex. Grandiosity often masks feelings of inadequacy, mediocrity, or a flawed self-image, with individuals striving to project perfection-hallmarks of narcissism. Two psychoanalytic models explore the origins of narcissistic personality disorder (NPD): Heinz Kohut’s self-psychology model and Otto Kernberg’s object-relations model. Both attribute NPD to inadequate parent-child relationships. Kernberg described NPD as stemming from emotionally distant, critical mothers, leading children to develop a grandiose ego as a defense against emotional neglect. This ego integrates the child’s perceived strengths, an exaggerated self-image, and an idealized view of a protective mother. Kohut suggested that NPD results from a developmental disruption in childhood, where natural narcissism fails to evolve, leaving the child trapped in a self-centered perspective.¹
Attachment theory explores the relationship between children and their primary caregivers, identifying four attachment styles: secure, disorganized, avoidant, and ambivalent. Research shows that attachment styles become evident as early as one year of age, with approximately 60% of the population forming secure attachments and the remaining 40% exhibiting problematic styles. Disorganized, avoidant, or ambivalent attachment styles are common in children of narcissistic caregivers, with disorganized attachment being particularly prevalent among individuals with NPD.²
Expanding on theories of narcissism, Pincus and Lukowitsky proposed a hierarchical model of pathological narcissism.³ They conceptualized pathological self-centeredness as a combination of three psychodynamic factors: dysfunctional self-regulation, emotion regulation, and interpersonal relationships. Their model places narcissism on a continuum, ranging from grandiose, entitled, and bold narcissism to vulnerable, sensitive, and shame-prone narcissism characterized by emotional turmoil, low self-esteem, and social withdrawal. This vulnerability manifests in emotions such as anger, envy, aggression, and even suicidality.⁴ While empirical evidence remains limited, Pincus and Lukowitsky suggest that both grandiose and vulnerable narcissism can present overtly or covertly.⁵
According to DSM-5 Narcissistic personality disorder can be defined as prevalent pattern of sense of grandiosity, self-love, astonishment when expected praise not impending, fantasies of power and success, feeling oneself unique, special, talented and gifted up to the level that even their essentials different to others, too much sure about their doings, lack of empathy and rationalize that others are concerned just about their own feelings, problems, needs and welfare, excessive self-admiration and boasting, arrogant and envious to others but justify that others are resentful and jealous. Nine indications cover the narcissistic diagnostic domain, five or more symptoms requisite for identification of egotistic features.6 Prevalence rates vary from 0% to 5.3% in community samples and from 1% to 17% in clinical settings. Features of NPD, such as grandiosity or self-loathing, social extroversion or isolation, and a propensity for antisocial behaviors, are more frequently identified in men, with 50–75% of cases involving males.⁷ While NPD is commonly observed in adolescents, it has also been diagnosed in preadolescents and is the second most reported personality disorder after antisocial personality disorder.⁸
Narcissism involves two main strategies to maintain inflated self-views: intrapsychic and interpersonal. Intrapsychically, self-admiration is linked to fantasies of success and power, characterized as a self-serving bias where individuals credit themselves for success and blame others for failure.⁹ NPD often co-occurs with other disorders, particularly substance use disorders, bipolar disorder, and personality disorders such as antisocial, histrionic, borderline, schizotypal, and passive-aggressive personality disorders.¹⁰ Additionally, depression and anxiety are common comorbidities in individuals with NPD, with grandiosity often linked to substance abuse.¹¹,¹² NPD is more frequently diagnosed in younger, unmarried males, with substance abuse, particularly cocaine, contributing to narcissistic traits. A study using the Narcissistic Personality Inventory (NPI) demonstrated a higher prevalence of narcissism among men compared to women.¹³,¹⁴
Although personality disorder assessment tools are widely available globally, indigenous tools tailored to the local context are lacking in Pakistan. The diversity of languages in Pakistan poses additional challenges, as not everyone is proficient in English, making it difficult for many to comprehend or communicate effectively. Thus, there was a pressing need to develop an Urdu-language tool to address cultural, linguistic, and comprehension barriers in assessing NPD among Pakistani adults. This self-report measure, constructed in Pakistan’s national language, is designed to be accessible not only to researchers and clinicians but also to laypersons.
To achieve these objectives, the study was conducted in two phases. The first phase involved developing an indigenous scale for NPD by creating and refining relevant items. The second phase focused on evaluating the psychometric properties of the developed scale.
METHODS
The study received ethical approval from the Departmental Research Review Committee (DRRC), Department of Psychology, University of Gujrat, Pakistan. It was conducted from February 15, 2019, to June 20, 2019, using a cross-sectional analytical design. Data were collected from various government and private colleges, universities, hospitals, and communities in Gujrat, Pakistan.
Inclusion and exclusion criteria: Participants included adults aged 19 years and above, both male and female. Individuals younger than 19 years and psychiatric patients were excluded.
Data collection: A 5-point Likert scale was used, ranging from "Strongly Agree (5)" to "Strongly Disagree." 15 Purposive sampling was employed due to time constraints. The study began with rapport building, where participants were informed about the study's objectives and assured of anonymity and confidentiality. Written and oral informed consent was obtained. Data were collected using a self-administered questionnaire with clear instructions provided to respondents.
Scale development procedure of Narcissistic personality disorder: A standardized scale development procedure was employed, starting from item pool generation to finalizing the scale.¹⁶ Initially, an item pool of 75 questions was created through a rigorous review of narcissistic personality disorder, drawing on sources such as the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), existing literature, and expert opinions using both inductive and deductive approaches. These items were designed to reflect individual thoughts, feelings, behaviors, interactions, and actions associated with narcissistic personality disorder.
An expert evaluation meeting was conducted to refine the item pool, where a panel of five PhD experts in the relevant field assessed each question for its essentiality, relevance to adults, and alignment with the construct of narcissistic personality. Following this analysis, 71 items were finalized for a preliminary tryout. A pilot study was then conducted to assess participants' comprehension of the newly developed test. The test was administered to 104 participants, and the data collected during the pilot study was used to calculate item-total correlations. Items with correlation coefficients below 0.4 were discarded, leaving 44 questions with coefficients greater than 0.40. Sixteen ambiguous items were excluded after this process.
The final data collection adhered to ethical research standards, including obtaining informed consent, ensuring confidentiality, providing debriefings, and maintaining research integrity. The finalized scale was administered to 234 adults (Male = 124, Female = 110), comprising both clinical (n = 100) and non-clinical (n = 134) participants aged 19 years and above. Participants were recruited from community, educational, and health institutions.
Subsequently, the psychometric properties of the newly developed scale were established. Data analysis included correlation analysis, exploratory factor analysis, confirmatory factor analysis, and reliability testing. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS-21) and Analysis of Moment Structures (AMOS-21).
RESULTS
The initial item pool of 75 was abridged to 71 by process of content validity. After pilot study, only 44 items were retained and these items were used in the final administration and a total of 234 participants responded to the questionnaire. Exploratory factor analysis assisted to delete d out non-significant items of the scale. In table II, the factor loading value was suppressed to 0.40 and literature suggests items containing value of 0.40 or >0.40 are considered appropriate. 17
Exploratory factor analysis revealed 9 factors which described 67.09% variance. Items with factor stuffing <0.4 were abolished, and items having values from .40 to .79 were retained. As there should be eight factors to better meet all the criteria mentioned in DSM-5.
Table III shows Kaiser-Meyer-Olkin measure of sampling adequacy i.e., 0.918; a significant Bartlett’s test of sphericity i.e., p<.001. Predominantly, factors labelled with 67.09% variance. Questions which are factor loaded with a value <0.4 were eliminated, and the items ranging from 0.40 to 0.81 were kept.
Drawing out 8 factors consequently by running EFA, it deemed to 7 factors by executing Amos Graphics 7. Each domain has different quantity of questions ranging two to four questions per factor.
CFA confirmed seven factors instead of eight by merging four signs into two domains; lack of empathy and relational explosiveness were merged in one group and arrogance and sense of power were sorted in one category. Two other categories revolve around self-grandiosity. It revealed that people have greater sense of magnificence about themselves.
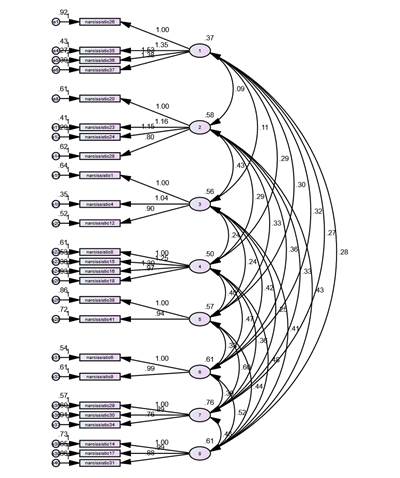
Item number 26, 35, 36, 37 were found to be reliable for the factor I. Further, 20, 23, 24, 28 number items were considered reliable for factor II. Item numbers 1, 4, 12 were found reliable for factor III. The item numbers 8, 15, 16, 18 were confirmed to be reliable for factor IV. Additionally, at factor V the item numbers 38, 41 were reliable. The item numbers 6, 9 were confirmed to be reliable for factor VI and item number 29, 30, 34 were included in factor VII. Finally, item number 14, 17, 31 were found reliable for factor VIII. Figure 1 depicts the pictorial explanation of confirmatory factor analysis of narcissistc personality disorder scale.
To fit the model CFI appropriately, modification indices were investigated. The indication of doubtful items through regression weight was the provision to omission. The analysis showed that 19 questions were found problematic and deletion of items leads to the better CFI value establishment. To better support the scale various items were cancelled i.e., 2, 3, 5, 7, 10, 11, 13, 19, 21, 22, 25, 27, 32, 33, 39, 40, 42, 43, and 44. Hence, 25-items questionnaire was finalized. The value of Comparative Fit Index (CFI) was 0.926 which suggested that model of goodness of fit is absolute fit and significant <0.001 (Table IV). The value of CFA above 0.90 is considered as appropriate. Results confirmed the model fit of the scale for narcissistic personality disorder scale.18
Reliability might be determined in various ways, yet the most normally acknowledged measure is assessing scale's internal consistency that is Cronbach's alpha which tells how well the things measure a similar construct. After the exploratory and confirmatory factor analysis have been directed illogical questions have been erased. A significant coefficient alpha (0.70) gives a sign areas of strength for covariance or homogeneity and recommends that the sample has been adequately recruited (Churchill, 1979). This step is validate on the grounds that the unidimensionality of scales has been established through the factor analysis. Reporting internal reliability ought to be viewed as totally important.The chronbach alpha reliability of the current scale was 0.922 which is a significant value (Table V). The reliability of the sub-scales was also significant (Table VI).19
Evidence of construct validity can be achieved by inspecting the degree to which the scales correspond with different measures intended to survey comparative builds (convergent validity) and to which they don't connect with unique measures (discriminant validity).20 To estimate the convergent validity of Narcissistic Personality Disorder Scale, convergent measure named translated version of SD3 (Short measure of Dark Triads)21, 22 subscales Narcissism assessing self-grandiosity was administered and resultant value was 0.570 which is a statistically significant value (Table VII). The final scale is attached in Annexure.
Table I: Correlation of 44 Items of Narcissistic personality disorder (n=104)
|
Sr. No. |
Item No. |
R |
Sr. No. |
Item No. |
R |
|
1 |
1 |
.427** |
23 |
25 |
.489** |
|
2 |
2 |
.556** |
24 |
26 |
.578** |
|
3 |
5 |
.598** |
25 |
28 |
.572** |
|
4 |
6 |
.521** |
26 |
30 |
.466** |
|
5 |
7 |
.519** |
27 |
31 |
.431** |
|
6 |
8 |
.493** |
28 |
32 |
.430** |
|
7 |
9 |
.608** |
29 |
33 |
.497** |
|
8 |
10 |
.505** |
30 |
35 |
.513** |
|
9 |
11 |
.531** |
31 |
36 |
.515** |
|
10 |
12 |
.540** |
32 |
37 |
.480** |
|
11 |
13 |
.578** |
33 |
39 |
.564** |
|
12 |
14 |
.434** |
34 |
40 |
.416** |
|
13 |
15 |
.632** |
35 |
41 |
.454** |
|
14 |
16 |
.655** |
36 |
43 |
.530** |
|
15 |
17 |
.630** |
37 |
44 |
.506** |
|
16 |
18 |
.702** |
38 |
47 |
.556** |
|
17 |
19 |
.444** |
39 |
49 |
.536** |
|
18 |
20 |
441** |
40 |
51 |
.561** |
|
19 |
21 |
.607** |
41 |
52 |
.437** |
|
20 |
22 |
.424** |
42 |
53 |
.493** |
|
21 |
23 |
.507** |
43 |
54 |
.532** |
|
22 |
24 |
.542** |
44 |
55 |
.502** |
**. Correlation is significant at the 0.01 level (2-tailed)
Item total correlation shows how highly correlated each item is with the overall scale. Ferkeitch (1991) suggested that correlation of correlated items should be ranged from 0.30 and 0.70 for a good scale. The analysis indicated that item total correlation of the current scale ranged from 0.42 to 0.70 which is well supported by literature (Table I).
Table II: Factor Loading of 43 Item on Narcissistic personality disorder scale
after Varimax Rotation (n=234)
|
Sr .No. |
Item No. |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
|
1 |
26 |
.593 |
|
|
|
|
|
|
|
|
|
2 |
32 |
.600 |
|
|
|
|
|
|
|
|
|
3 |
33 |
.606 |
|
|
|
|
|
|
|
|
|
4 |
35 |
.736 |
|
|
|
|
|
|
|
|
|
5 |
36 |
.779 |
|
|
|
|
|
|
|
|
|
6 |
37 |
.792 |
|
|
|
|
|
|
|
|
|
7 |
39 |
.723 |
|
|
|
|
|
|
|
|
|
8 |
43 |
.574 |
|
|
|
|
|
|
|
|
|
9 |
20 |
|
.737 |
|
|
|
|
|
|
|
|
10 |
21 |
|
.521 |
|
|
|
|
|
|
|
|
11 |
22 |
|
.504 |
|
|
|
|
|
|
|
|
12 |
23 |
|
.788 |
|
|
|
|
|
|
|
|
13 |
24 |
|
.791 |
|
|
|
|
|
|
|
|
14 |
25 |
|
.734 |
|
|
|
|
|
|
|
|
15 |
28 |
|
.536 |
|
|
|
|
|
|
|
|
16 |
1 |
|
|
.681 |
|
|
|
|
|
|
|
17 |
2 |
|
|
.762 |
|
|
|
|
|
|
|
18 |
3 |
|
|
.599 |
|
|
|
|
|
|
|
19 |
4 |
|
|
.569 |
|
|
|
|
|
|
|
20 |
11 |
|
|
.551 |
|
|
|
|
|
|
|
21 |
12 |
|
|
.626 |
|
|
|
|
|
|
|
22 |
13 |
|
|
.538 |
|
|
|
|
|
|
|
23 |
8 |
|
|
|
.542 |
|
|
|
|
|
|
24 |
15 |
|
|
|
.514 |
|
|
|
|
|
|
25 |
16 |
|
|
|
.651 |
|
|
|
|
|
|
26 |
18 |
|
|
|
.671 |
|
|
|
|
|
|
27 |
38 |
|
|
|
|
.567 |
|
|
|
|
|
28 |
40 |
|
|
|
|
.622 |
|
|
|
|
|
29 |
41 |
|
|
|
|
.516 |
|
|
|
|
|
30 |
42 |
|
|
|
|
.482 |
|
|
|
|
|
31 |
44 |
|
|
|
|
.403 |
|
|
|
|
|
32 |
5 |
|
|
|
|
|
.576 |
|
|
|
|
33 |
6 |
|
|
|
|
|
.504 |
|
|
|
|
34 |
7 |
|
|
|
|
|
.544 |
|
|
|
|
35 |
9 |
|
|
|
|
|
.495 |
|
|
|
|
36 |
10 |
|
|
|
|
|
.495 |
|
|
|
|
37 |
29 |
|
|
|
|
|
|
.702 |
|
|
|
38 |
30 |
|
|
|
|
|
|
.618 |
|
|
|
39 |
34 |
|
|
|
|
|
|
.563 |
|
|
|
40 |
14 |
|
|
|
|
|
|
|
.451 |
|
|
41 |
17 |
|
|
|
|
|
|
|
.481 |
|
|
42 |
31 |
|
|
|
|
|
|
|
.562 |
|
|
43 |
27 |
|
|
|
|
|
|
|
|
.689 |
Extraction Method: Principal Component Analysis. Rotation Method Varimax with Kaiser Normalization. Note : (Values<.4 are suppressed)
After running exploratory factor analysis 9 factors were extracted with 67.09% variance. Items with factor loading <0.4 were abolished, and items having values from .40 to .79 were retained (Table II).
|
Table III: Kaiser-Meyer-Olkin (KMO) and Bartlett’s test of sphericity (n=234)
|
||||
|
Varaible |
KMO |
Bartlett’s Test |
||
|
df |
Sig |
|||
|
Narcissistic Personality Disorder Scale (NPDS) |
.918 |
6642.386 |
946 |
.000 |
Table III shows Kaiser-Meyer-Olkin measure of sampling adequacy i.e., 0.918 which is significant and Bartlett’s test of sphericity is also significant i.e., p <.001.
Table IV: Model fit summary of confirmatory factor analysis (n=234)
|
P Value |
CMIN/DF |
GFI |
AGFI |
CFI |
RMSEA |
RMR |
|
.000 |
1.775 |
.870 |
.829 |
.926 |
.058 |
.065 |
CMIN/DF: chi-square minimum/degree of freedom; GFI: Goodness of Fit Index; CFI: Comparative Fit Index, AGFI: Adjusted Goodness of Fit Index; RMSEA: Root Mean Square of Error Approximation
The value of CFA above 0.90 is considered as appropriate. Hence, the scale results depicted that CFI = 0.926, GFI = .870 and AGFI = .829 which suggested that model of goodness of fit is absolutely fit and significant i.e., <0.001 (Table IV).
|
|
Figure 1: Confirmatory factor analysis resulted in 25 item Narcissistic Personality Disorder Scale
|
Table V: Cronbach alpha of Narcissistic personality disorder scale (n=234) |
||||
|
Scale |
Cronbach’s Alpha |
Number of Items |
Sig |
|
|
Narcissistic Personality Disorder Scale (NPDS) |
.922 |
25 |
.000 |
|
The reliability of the narcissistic personality disorder scale expressed α=.922. The cut-off value for significantly high reliability is 0.70 and above as per literature (Table V).
|
Table VI: Cronbach alpha of subscales of Narcissistic personality disorder scale (n=234)
|
|
Subscales |
Total items |
Cronbach Alpha |
|
1. Interpersonally exploitive behaviour |
4 |
.724 |
|
2. Grandiose self-importance |
4 |
.826 |
|
3. Excessive self-admiration |
3 |
.764 |
|
4. Distinctiveness |
4 |
.803 |
|
5. Envious to others |
2 |
.574 |
|
6. Feeling of uniqueness |
2 |
.676 |
|
7. Arrogance and sense of entitlement |
3 |
.708 |
|
8. Fantasy feelings |
3 |
.673 |
|
Note: p<.01 |
|
|
There are eight subscale of narcissistc personality disorder. Reliability analysis was administered on each scale using SPSS which is as follows: Interpersonally exploitive behaviour =.724, Grandiose self-importance = .826, Excessive self-admiration =.764, Distinctiveness =.803, Envious to others =.574, Feeling of uniqueness =.676, Arrogance and sense of entitlement =.708 and Fantasy feelings=.673. The reliability of all the subscale is significantly high which depicted that this is a consistent measure to assess the narcissistic personality disorder in adults (Table VI).
Table VII: Validity analysis of narcissistic personality disorder scale (n=55)
|
Scales |
1 |
2 |
3 |
|
1. Narcissistic |
- |
|
|
|
2. SD3-N |
.570** |
- |
|
Note: ** p<.01 SD3=Triad subscale Narcissism (SD3)
Triad subscale narcissism comprised of 9-items scale which is used to assess the narcissism personality disorder. The convergent validity of the narcissism personality disorder scale with the well-developed SD3 was conducted and resultant value is .570 which is a appropriate value to prove a measure as psychometrically sound (Table VII).
Operational definition: Narcissistic personality disorder is a mental health condition which is characterized by a life-long pattern of exaggerated feelings of self-importance. In this condition individual has Interpersonally exploitive behavior, pervasive pattern of grandiosity, need for excessive self-admiration and feeling of being unique and distinctive from others. These individual are entitled to attention or approval from others. Furthermore, individuals with this condition are enviousness to others and show arrogant and haughty behaviors toward others.
Having narcissistic tendencies are normal when they occur occasionally but, persistent occurance of all these conditions lead to the abnormality of behavior and known as narcissistic personality disorder.
Narcissistic personality disorder self-rating scale (English & Urdu versions) are given as Annexures (Appendix 1 & 2).
DISCUSSION
This study aimed to develop and validate a scale for assessing Narcissistic Personality Disorder (NPD). An initial pool of 75 items was refined through content validity, pilot testing, and exploratory factor analysis (EFA), resulting in a 44-item questionnaire administered to 234 participants. EFA identified nine factors accounting for 67.09% variance, with factor loadings ranging from 0.40 to 0.79. Confirmatory factor analysis (CFA) further refined the scale, merging factors to produce a seven-factor model comprising 25 items. Reliability testing revealed a Cronbach’s alpha of 0.922 for the overall scale, with subscale reliabilities ranging from 0.574 to 0.826. Convergent validity with the SD3 Narcissism subscale yielded a statistically significant value of 0.570. These findings confirm the scale as a psychometrically sound instrument for assessing narcissistic personality traits, with high internal consistency and validity.
Narcissism is a predominant personality trait characterized by grandiosity, self-love and lack of remorse for others. Acoording to Kernberg, Narcissism associated with need of constant admiration and reassurance that they are uniquely special. It was observed that the sense of entitlement and sense of superiority leads to others’ exploitation. Moreover, narcissism and high self-esteem are independent constructs and that narcissism correlates with other pathological and irrational behavior.23
Although personality has been the focus of attention for psychologists, clinicians, psychoanalysts, psychiatrists and researchers as well for many years. Some presented personality theories, some focused on personality patterns or styles, some others presented stages of personality development and many more. Every new exertion has its own worth and reveals some more aspects that either may be neglected or ignored by other contributors.
In the past 40 years, narcissistic personality has gained much attention. Various instruments and approaches constructed and presented to diagnose and detect personality disorder. Literature revealed the richness of personality disorders assessment measures across the countries. There are numerous theories, researches, reliable and valid measures available to measure the personality disorders, across different territories. Scales are not just developed in English, international language, but also translated into different language e.g., German, Korean, Spanish and Chinese languages. There are some measures available which differentiate between pathological/clinical and normal narcissism. All these tests are established in foreign language. So for filling the gape local NPD scale was developed.
Thomaes, Stegge, Bushman, Olthof, and Denissen (2008) constructed and authenticated a short but comprehensive gauge for measurement of childhood narcissism consist of 10 items. The scale was named as Childhood Narcissism Scale (CNS) and administered on 8 to 14 years children. The main objective of the scale was to measure individual differences in childhood narcissism. The study was divided into six studies. First study was based on selection of items. Second and third studies was conducted on Dutch and American participants respectively. Fourth study was grounded on internal consistency and its internal consistency and test-retest reliability (time interval of 2-6 months). Fifth study was conducted to explore relationship of childhood narcissism and self-esteem and sixth study led to find relation of childhood narcissism and empathy as well as aggression. Initial item pool was comprised of 48 items that was abridged to 10 items. Results revealed that the relationship of childhood narcissism was not related to self-esteem. But the relation with self-love or appraisal, social appraisal apprehension and self-worth eventuality, a genetic interactive goal, and emotive extreme was positive. Moreover, CNS is positively correlated to aggression that is due to the ego threat and negatively correlated to empathic apprehension. The outcomes also suggested that just like adult narcissism childhood narcissism also has alike psychological and interpersonal associates. Finally, after passing through all phases of scale development of CNS, a scale with strong psychometric properties, a measuring instrument of narcissism in children and young adolescents provides to researchers.24
Five Factor Narcissism Inventory (FFNI) developed in 2012 (Glover et al., 2012). There are 148 items grouped into 15 narcissism trait scales, containing Reactive Anger, Shame, Indifference, Need for Admiration, Exhibitionism, Thrill-Seeking (symbolised in the EPA; Lynam et al., 2011), Cynicism/Distrust, Authoritativeness, Grandiose Fantasies, Manipulativeness, Lack of Empathy, Exploitative behavior, Arrogance, Entitlement, and Acclaim-Seeking. Above mentioned 15 different scales provide a comprehensive description of narcissistic pathology. It was constructed in English language and 5-point response scale “1” strongly disagree to “5” strongly agree was used.25
Pincus, Ansell, Pimentel, Cain, Wright, and Levy (2009) constructed The Pathological Narcissism Inventory (PNI). The main objective of the test was to differentiate between pathological/clinical and normal narcissism. It encompassed two predominant dimensions with 52 items i.e., narcissistic grandiosity and narcissistic vulnerability. Narcissistic grandiosity includes four pathological features; entitlement rage, grandiose fantasy, exploitative behavior, and self-sacrificing self-enhancement. Whereas, Narcissistic vulnerability includes three aspects: hiding the self, contingent self-esteem, and devaluing. PNI is analogous to Murray’s conception of narcissism focus on both overt and covert behaviours. Murray’s Narcissism Scale (1938), 20-item self-report scale that assess narcissism; overt and covert feelings of insecurity, and grandiose behaviour.26
In order to develop scale and establish psychometric properties several steps were followed. These steps included: item pool generation, content validity, try out, final administration, exploratory and confirmatory factor analysis. Exploratory factor analysis expressed 9 domains with certain acceptable values like KMO >.9 value i.e., .918, i.e. satisfactory value with 67.09% variance and loading of facet within ranges .40 and .79. Subsequently, confirmation proceeded with execution of regression weights in modification indices. 25 items out of 43, with 18 discarded question, was the final measure having >0.9 CFI value, >0.8 GFI, <2 CMIN/DF and equivalent to 0.05 RMSEA value i.e., .926, .870, 1.775 and .05 respectively. It depicts the satisfactory fit model. Significant positive correlation has been evaluated between Narcissistic Personality Disorder Scale and Short Dark Triad subscale Narcissism (SD3),et17 translated into Urdu language,18 as r = .570** and negative correlation with Rosenberg Self-Esteem Scale as r = -.059. Reliability outcome showed good values α = .922. Finally, 25-items questionnaire was established.
CONCLUSION
The Indigenous Narcissistic Personality Disorder Scale (NPDS), comprising 25 questions and 7 sub-scales, was developed in the native language of Pakistan, Urdu. This reliable and efficient diagnostic tool is designed to evaluate narcissistic personality traits and can be utilized by researchers, psychologists, psychiatrists, social workers, and other mental health professionals. Aligned with DSM-5 criteria, the NPDS demonstrates strong psychometric properties, including high reliability and construct validity, making it valuable for clinical and research purposes. Future studies should investigate its applicability across diverse populations to broaden its utility.
Limitation of the study and suggestion
Further validation studies are needed to enhance the psychometric robustness of the scale. Additionally, translating and adapting the scale into other languages would facilitate its use on an international level. To improve its applicability in psychiatric settings, more data should be collected from clinical samples.
REFERENCES
1. Schmidt A. Comparison of kernbergs and kohuts theory of narcissistic personality disorder. Turk Psikiyatri Derg 2019;30(2):137-41.
2. Meyer B, Pilkonis PA. Attachment Theory and Narcissistic Personality Disorder. The handbook of narcissism and narcissistic personality disorder: Theoretical approaches, empirical findings, and treatments. Publisher: Hoboken, NJ: John Wiley and Sons. 2012; 434-44. https://doi.org/10.1002/9781118093108.ch39
3. Pincus AL, Lukowitsky MR. Pathological narcissism and narcissistic personality disorder. Annu Rev Clin Psychol 2010;6:421-46. https://doi.org/10.1146/annurev.clinpsy.121208.131215
4. Pincus AL. The pathological narcissism inventory, in understanding and treating pathological narcissism. Am Psychol Assoc 2013;93-110. https://psycnet.apa.org/doi/10.1037/14041-006
5. Schalkwijk F, Luyten P, Ingenhoven T, Dekker J. Narcissistic personality disorder: Are psychodynamic theories and the alternative DSM-5 model for personality disorders finally going to meet? Front Psychol 2021;12:676733. https://doi.org/10.3389/fpsyg.2021.676733
6. American Psychiatric Association. Diagnostic Statistical Manual for Mental Disorders. 5th ed. Arlington, V.A: American Psychiatric Publications 2013; 669-71.
7. Caligor E, Levy KN, Yeomans FE. Narcissistic personality disorder: Diagnostic and clinical challenges. Am J Psychiatry 2015;172(5):415-22. https://doi.org/10.1176/appi.ajp.2014.14060723
8. Bardenstein KK. The cracked mirror: Features of narcissistic personality disorder in children. Psychiatr Ann 2009;39(3):147-55. https://doi.org/10.3928/00485713-20090301-01
9. Campbell WK, Reeder GD, Sedikides C, Elliot AJ. Narcissism and comparative self-enhancement strategies. J Res Pers 2000;34(3):329–47. https://doi.org/10.1006/jrpe.2000.2282
10. Ronningstam EF, Weinberg I. Narcissistic personality disorder: progress in recognition and treatment. Focus 2013;11(2):167-77. http://dx.doi.org/10.1176/appi.focus.11.2.167
11. Pincus AL, Lukowitsky MR. Pathological narcissism and narcissistic personality disorder. Annu Rev Clin Psychol 2010;6:421-46. https://doi.org/10.1146/annurev.clinpsy.121208.131215
12. Russ E, Shedler J, Bradley R, Westen D. Refining the construct of narcissistic personality disorder: Diagnostic criteria and subtypes. Am J Psychiatry 2008;165(11):1473-81. https://doi.org/10.1176/appi.ajp.2008.07030376
13. Stinson FS, Dawson DA, Goldstein RB, Chou SP, Huang B, Smith SM. et al. Prevalence, correlates, disability, and comorbidity of DSM-IV narcissistic personality disorder: results from the wave 2 national epidemiologic survey on alcohol and related conditions. J Clin Psychiatry 2008;69(7):1033–45. https://doi.org/10.4088/jcp.v69n0701
14. Grijalva E, Newman DA, Tay L, Donnellam M, Harms PD, Robins RW, et al. Gender differences in narcissism: a meta-analytic review. Psychol Bull 2015;141(2):261-310. https://doi.org/10.1037/a0038231
15. Likert R. A technique for the measurement of attitudes. Arch Psychol 1932;22(140):5-55.
16. Tay L, Jebb A. Scale Development. In S. Rogelberg (Ed), The SAGE Encyclopaedia of Industrial and Organizational Psychology. 2nd ed. Thousand Oaks, CA: Sage; 2017.
17. Rahn M. Factor Analysis: A Short Introduction, Part 5–Dropping unimportant variables from your analysis 2018. [Accessed on: June 30, 2019]. Available from URL: https://www.theanalysisfactor.com/fa ctor-analysis-5/
18. Zainudin A. A Handbook on SEM: Structural equation modelling using amos graphics. 4th ed. Validating the Measurement Model: CFA 2012:54-73.
19. Gliem JA, Gliem RR. Calculating, interpreting, and reporting cronbach’s alpha reliability coefficient for likert-type scales. Midwest research to practice conference in adult, continuing, and community education. 2003. [Accessed on: June 30, 2019]. Available from URL: http://hdl.handle.net/1805/344
20. Hinkin TR, Tracey JB, Enz CA. Scale Construction: Developing Reliable and Valid Measurement Instruments. J Hosp Tour Res 1997;21(1):100-20. https://doi.org/10.1177/109634809702100108
21. Jones DN, Paulhus DL. Introducing the short Dark Triad (SD3): a brief measure of dark personality trait. Assessment 2014;21(1):28–41. https://doi.org/10.1177/1073191113514105
22. Gul-e-Sehar, Fatima I. Dark triad personality traits as predictors of bullying and victimization in adolescents. J Behav Sci 2016;26(1):51-65.
23. Thomaes S, Bushman BJ, Stegge H, Olthof T. Trumping shame by blasts of noise: narcissism, self-esteem, shame, and aggression in young adolescents. Child Dev 2008;79(6):1792-801. https://doi.org/10.1111/j.1467-8624.2008.01226.x
24. Thomaes S, Stegge H, Bushman BJ, Olthof T, Denissen J. Development and validation of the childhood narcissism scale. J Pers Assess 2008;90(4):382-91. https://doi.org/10.1080/00223890802108162
25. Glover N, Miller JD, Lynam DR, Crego C, Widiger TA. The five-factor narcissism inventory: a five-factor measure of narcissistic personality traits. J Pers Assess 2012;94(5):500-12. https://doi.org/10.1080/00223891.2012.670680
26. Pincus AL, Ansell EB, Pimentel CA, Cain NM, Wright AGC, Levy KN. Initial construction and validation of the pathological narcissism inventory. Psychol Assess 2009;21(3):365-79. https://doi.org/10.1037/a0016530
|
Following author have made substantial contributions to the manuscript as under:
SR & ZB: Conception and study design, acquisition, analysis and interpretation of data, drafting the manuscript, critical review,approval of the final version to be published
Author agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST Authors declared no conflict of interest, whether financial or otherwise, that could influence the integrity, objectivity, or validity of their research work.
GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |
APPENDIX 1
Narcissistic Personality Disorder Scale
Test Instructions
Item Scoring Format
1 = Strongly Disagree. 2 = Disagree. 3 = To some extent. 4 = Agree. 5 = Strongly Agree.
*No reverse scoring for any item.
|
Subscales |
Item No. |
Total items |
|
1. Interpersonally exploitive behavior |
1-4 |
4 |
|
2. Grandiose self-importance |
5-8 |
4 |
|
3. Excessive self-admiration |
9-11 |
3 |
|
4. Distinctiveness |
12-15 |
4 |
|
5. Envious to others |
16-17 |
2 |
|
6. Feeling of uniqueness |
18-19 |
2 |
|
7. Arrogance and sense of entitlement |
20-22 |
3 |
|
8. Fantasy feelings |
23-25 |
3 |
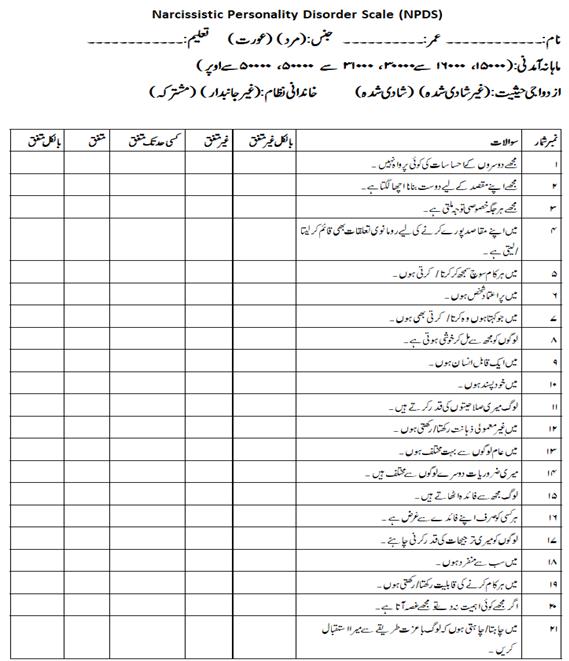
APPENDIX 2