![]() https://doi.org/10.35845/kmuj.2025.23319 ORIGINAL
ARTICLE
https://doi.org/10.35845/kmuj.2025.23319 ORIGINAL
ARTICLE
Development and Psychometric Validation of the Urdu-language
Antisocial Personality Disorder Scale for Adults
Samia Rashid ![]() 1,
2, Zaqia Bano
1,
2, Zaqia Bano ![]() 2,
3
2,
3
|
1: Department of Psychology, University of Gujrat, Gujrat, Pakistan 2: Department of Psychology, National University of Medical Sciences, Rawalpindi, Pakistan 3: Department of Clinical Psychology, NUR International University, Lahore, Pakistan
Email
Contact #: +92-347- 6681017
Date Submitted: February 07, 2023 Date Revised: July 09, 2024 Date Accepted: August 03, 2024 |
|
THIS ARTICLE MAY BE CITED AS: Rashid S, Bano Z. Development and Psychometric Validation of the Urdu-language Antisocial Personality Disorder Scale for Adults. Khyber Med Univ J 2025;17(Suppl 1):S28-S36. https://doi.org/10.35845/kmuj.2025.23319 |
ABSTRACT
Objective: To develop an Antisocial Personality Disorder Scale (ASPDS) for adults in Urdu language and evaluate its psychometric properties.
Methods: A cross-sectional analytical study was conducted from February 15 to June 20, 2019, on 234 adults (18-60 years) from different institutions of Gujrat, Pakistan,. The ASPDS was developed through diagnostic criteria, literature review, and expert validation, with an initial pool of 91 items tested on 104 adults, refined to 66 items. Exploratory Factor Analysis (EFA) identified seven factors, excluding items with factor loadings below 0.4. Confirmatory Factor Analysis (CFA) validated the seven-factor structure, resulting in a 28-item scale. Reliability was assessed using Cronbach’s alpha, and convergent validity was established by correlating ASPDS scores with the psychopathy subscale of Short Measure of Dark Triads (SD3).
Results: EFA identified seven factors explaining 62.35% of the variance, with factor loadings ranging from 0.44 to 0.73. CFA confirmed the model fit (CFI = 0.917, RMSEA = 0.063), and the final ASPDS comprised 28 items. The scale demonstrated high internal consistency, with a Cronbach’s alpha of 0.94 and subscale reliabilities ranging from 0.67 to 0.91. Convergent validity was confirmed by a significant correlation (r =0.692, p <0.01) with the SD3 psychopathy subscale. The Kaiser-Meyer-Olkin measure was 0.93, and Bartlett’s test of sphericity was significant (p <0.001). Data were analyzed using SPSS-21 and AMOS-21.
Conclusion: ASPDS is a reliable and valid tool for assessing antisocial personality disorder among adults. Its strong psychometric properties and alignment with established measures support its utility in clinical and research settings.
Keywords: Personality Assessment (MeSH); Antisocial Personality Disorder (MeSH); Scale development (Non-MeSH); Scale validation (Non-MeSH).
INTRODUCTION
Antisocial personality disorder (ASPD) is characterized by a disturbed disposition, marked by behaviours such as rule-breaking, violation of social norms, disrespect for others’ rights, physical and verbal aggression, reckless behaviour, and a lack of remorse or guilt, even in extreme cases such as harming others. Individuals with ASPD often exhibit irresponsibility, deceitfulness, and a willingness to harm others for personal gain. They are prone to physical confrontations, including with family members, and derive pleasure from betraying and disregarding others' well-being.¹
The term "antisocial behaviour" refers to dysfunctional actions, attitudes, and personality traits that frequently result in negative interpersonal and societal outcomes.² Despite advancements in theoretical and methodological approaches, there remains disagreement over the nature and scope of antisocial behaviour. Research in this field has often been inconsistent, with varying conceptual frameworks and methodologies, complicating the integration of findings and suggesting that the constructs may be distinct.³
Antisocial behaviours, if persistent, typically begin in childhood or adolescence and can extend into adulthood. These behaviours are initially recognized as oppositional defiant disorder in childhood, which can evolve into conduct disorder in adolescence and ultimately lead to ASPD in adulthood. Low socialization scores are a common indicator of ASPD in adulthood.⁴ Studies show that approximately 47% of individuals with ASPD have significant interactions with the criminal justice system.⁵ The term "antisocial personality disorder" was introduced by Philippe Pinel, a French physician, in response to the impulsive and damaging behaviour of his patients. Historically, ASPD was referred to as psychopathy or sociopathy until the DSM-III in 1980, with both terms used interchangeably to describe individuals lacking empathy. While these terms share similarities, a key distinction exists: psychopaths lack morality and empathy, whereas sociopaths may have a conscience but one that is inconsistent with societal norms⁶. Antisocial behaviours exhibited before age 18 are classified as conduct disorder. However, if these behaviours persist into adulthood, they are diagnosed as ASPD⁷. Research indicates that ASPD is more prevalent in less-educated and lower-class populations⁸. ASPD affects an estimated 0.6% to 3.6% of adults, with men being three times more frequently affected than women. Co-occurring mental health disorders, such as depression, anxiety, bipolar disorder, and substance use disorders, are common among individuals with ASPD¹. Several measurement tools have been developed to assess antisocial behaviour, including the Antisocial Personality Questionnaire (APQ) by Blackburn and Fawcet, which is a self-report inventory consisting of 125 questions⁹. The Psychopathy Checklist (PCL) contains 22 items divided into two factors, each reflecting a distinct set of characteristics associated with psychopathy¹⁰.
Personality disorders, including ASPD, have long been a subject of debate in psychiatry and psychology. However, understanding dysfunction requires knowledge of the normal course of personality development. Cultural differences may influence psychological assessments, as most psychological exams, including those in Pakistan, are administered in English, which could lead to misinterpretation of results due to cultural variations. Cross-cultural assessment remains a complex issue, as standardized exams applied across different cultural contexts may not accurately measure psychological constructs due to cultural influences on personality traits. The purpose of the current study was to develop an Antisocial Personality Disorder Scale for adults in the Urdu language and to evaluate its psychometric properties.
METHODS
This study was conducted between February 15 and June 20, 2019, using a cross-sectional analytical study design. The study was approved by the Departmental Research Review Committee (DRRC) of the Psychology Department, University of Gujrat, Pakistan, after addressing ethical concerns. Data were collected from various government and private colleges, universities, hospitals, and community settings in Gujrat, Pakistan.
Scale development: The initial phase of the study focused on developing the Adult ASPDS using standardized methods for scale development. 11 Items were generated based on the diagnostic criteria for antisocial personality disorder, symptoms reported in the literature, and expert opinions. Items were formulated as ordinal-level statements, structured sequentially from weaker to stronger expressions, and presented in a multiple-choice format. These items aimed to capture thoughts, behaviours, and interpersonal relationships relevant to the disorder.
Content validation of the item pool was performed by subject specialists. Experts assessed each item for essentiality, appropriateness for adults, and relevance to the construct of personality disorders. After careful review, 91 items were finalized for initial testing.
Pilot testing: A purposive sampling technique was employed to recruit participants for the pilot phase, targeting individuals aged 18 and above from community, educational, and healthcare institutions. A total sample of 104 adults participated, providing consent before completing the scale. The scale was administered with a five-point Likert rating format: "Strongly Disagree" (1), "Disagree" (2), "To some extent" (3), "Agree" (4), and "Strongly Agree" (5). Reverse scoring was applied to reverse-worded items.
Pilot testing evaluated user understanding and identified potential issues with the items. Correlation analysis was conducted on item responses, and items with correlation coefficients below 0.40 were eliminated. The remaining 66 items demonstrated reliability and were retained for further validation.
Final administration: In the final administration phase, the refined 66-item scale was distributed to a sample of 234 participants aged 18 to 60 years, drawn from diverse settings including community centres, colleges, universities, and professional workplaces. Participants completed both the scale and a demographic form. Data analysis included item-total correlation, with items showing coefficients greater than 0.40 considered valid and reliable for inclusion in the final scale.
RESULTS
Table I: Correlation coefficient of 66 items of antisocial personality disorder (n=104)
|
Sr. No. |
Item No. |
R |
Sr. No. |
Item No. |
R |
|
1 |
1 |
.436** |
34 |
52 |
.463** |
|
2 |
2 |
.524** |
35 |
54 |
.603** |
|
3 |
3 |
.614** |
36 |
56 |
.441** |
|
4 |
4 |
.574** |
37 |
58 |
.460** |
|
5 |
5 |
.567** |
38 |
59 |
.528** |
|
6 |
7 |
.689** |
39 |
60 |
.508** |
|
7 |
8 |
.556** |
40 |
61 |
.608** |
|
8 |
9 |
.541** |
41 |
62 |
.738** |
|
9 |
10 |
.626** |
42 |
63 |
.714** |
|
10 |
12 |
.564** |
43 |
64 |
.646** |
|
11 |
13 |
.423** |
44 |
65 |
.576** |
|
12 |
18 |
.593** |
45 |
66 |
.614** |
|
13 |
19 |
.501** |
46 |
67 |
.603** |
|
14 |
21 |
.643** |
47 |
68 |
.536** |
|
15 |
25 |
.475** |
48 |
39 |
.691** |
|
16 |
26 |
.544** |
49 |
70 |
.660** |
|
17 |
27 |
.454** |
50 |
71 |
.742** |
|
18 |
30 |
.523** |
51 |
72 |
.648** |
|
19 |
31 |
.606** |
52 |
73 |
.627** |
|
20 |
32 |
.506** |
53 |
74 |
.658** |
|
21 |
33 |
.658** |
54 |
75 |
.637** |
|
22 |
34 |
.567** |
55 |
76 |
.492** |
|
23 |
35 |
.609** |
56 |
77 |
.532** |
|
24 |
36 |
.618** |
57 |
78 |
.642** |
|
25 |
37 |
.579** |
58 |
79 |
.490** |
|
26 |
38 |
.492** |
59 |
80 |
.404** |
|
27 |
42 |
.600** |
60 |
81 |
.662** |
|
28 |
44 |
.502** |
61 |
82 |
.421** |
|
29 |
46 |
.488** |
62 |
83 |
.586** |
|
30 |
48 |
.577** |
63 |
84 |
.524** |
|
31 |
49 |
.554** |
64 |
85 |
.478** |
|
32 |
50 |
.451** |
65 |
86 |
.516** |
|
33 |
51 |
.575** |
66 |
89 |
.499** |
**. Correlation is significant at the 0.01 level (2-tailed)
Exploratory factor analysis (EFA): Items with less than point four value i.e., <.4, were suppressed. Factor’s extraction was based on eigenvalue more than 1. Four factors were explored through data reduction, exploratory factor analysis.
Table II: Kaiser-Meyer-Olkin (KMO) and Bartlett’s test of sphericity (n=234)
|
Variable |
KMO |
Bartlett’s Test |
||
|
Chi-Square |
Df |
Sig |
||
|
Antisocial Personality Disorder Scale (APDS) |
.933 |
12584.627 |
2145 |
.000 |
Results indicated that Kaiser-Meyer-Olkin measure of sampling was adequate i.e., .93, and Bartlett’s test of sphericity was significant (p<.001).
Initially, 7 factors were explored on the basis of fixed number of factors, which describe 60.22% variance. Below .4 factor loading value items were eliminated, and factor loading ranging from .40 to .73.
Table III: Factor loading of 62 item on ASPDS after varimax rotation (n=234)
|
Sr. No. |
Item No. |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
1 |
23 |
.519 |
|
|
|
|
|
|
|
2 |
24 |
.587 |
|
|
|
|
|
|
|
3 |
25 |
.582 |
|
|
|
|
|
|
|
4 |
33 |
.462 |
|
|
|
|
|
|
|
5 |
35 |
.527 |
|
|
|
|
|
|
|
6 |
40 |
.513 |
|
|
|
|
|
|
|
7 |
41 |
.665 |
|
|
|
|
|
|
|
8 |
42 |
.697 |
|
|
|
|
|
|
|
9 |
43 |
.679 |
|
|
|
|
|
|
|
10 |
46 |
.442 |
|
|
|
|
|
|
|
11 |
48 |
.598 |
|
|
|
|
|
|
|
12 |
49 |
.573 |
|
|
|
|
|
|
|
13 |
50 |
.625 |
|
|
|
|
|
|
|
14 |
51 |
.675 |
|
|
|
|
|
|
|
15 |
52 |
.731 |
|
|
|
|
|
|
|
16 |
53 |
.712 |
|
|
|
|
|
|
|
17 |
54 |
.617 |
|
|
|
|
|
|
|
18 |
57 |
.432 |
|
|
|
|
|
|
|
19 |
60 |
.467 |
|
|
|
|
|
|
|
20 |
4 |
|
.608 |
|
|
|
|
|
|
21 |
7 |
|
.629 |
|
|
|
|
|
|
22 |
8 |
|
.477 |
|
|
|
|
|
|
23 |
9 |
|
.649 |
|
|
|
|
|
|
24 |
10 |
|
.493 |
|
|
|
|
|
|
25 |
13 |
|
.605 |
|
|
|
|
|
|
26 |
19 |
|
.584 |
|
|
|
|
|
|
27 |
21 |
|
.645 |
|
|
|
|
|
|
28 |
22 |
|
.506 |
|
|
|
|
|
|
29 |
27 |
|
.550 |
|
|
|
|
|
|
30 |
28 |
|
.678 |
|
|
|
|
|
|
31 |
29 |
|
.652 |
|
|
|
|
|
|
32 |
44 |
|
.550 |
|
|
|
|
|
|
33 |
45 |
|
.529 |
|
|
|
|
|
|
34 |
47 |
|
.585 |
|
|
|
|
|
|
35 |
64 |
|
.430 |
|
|
|
|
|
|
36 |
26 |
|
|
.460 |
|
|
|
|
|
37 |
39 |
|
|
.468 |
|
|
|
|
|
38 |
56 |
|
|
.589 |
|
|
|
|
|
39 |
58 |
|
|
.728 |
|
|
|
|
|
40 |
59 |
|
|
.605 |
|
|
|
|
|
41 |
61 |
|
|
.674 |
|
|
|
|
|
42 |
62 |
|
|
.473 |
|
|
|
|
|
43 |
63 |
|
|
.609 |
|
|
|
|
|
44 |
14 |
|
|
|
.536 |
|
|
|
|
45 |
15 |
|
|
|
.602 |
|
|
|
|
46 |
16 |
|
|
|
.661 |
|
|
|
|
47 |
17 |
|
|
|
.571 |
|
|
|
|
48 |
18 |
|
|
|
.543 |
|
|
|
|
49 |
38 |
|
|
|
.646 |
|
|
|
|
50 |
30 |
|
|
|
|
.511 |
|
|
|
51 |
31 |
|
|
|
|
.519 |
|
|
|
52 |
32 |
|
|
|
|
.408 |
|
|
|
53 |
36 |
|
|
|
|
.609 |
|
|
|
54 |
37 |
|
|
|
|
.613 |
|
|
|
55 |
66 |
|
|
|
|
.491 |
|
|
|
56 |
1 |
|
|
|
|
|
.618 |
|
|
57 |
2 |
|
|
|
|
|
.481 |
|
|
58 |
5 |
|
|
|
|
|
.615 |
|
|
59 |
6 |
|
|
|
|
|
.562 |
|
|
60 |
3 |
|
|
|
|
|
|
.719 |
|
61 |
12 |
|
|
|
|
|
|
.474 |
|
62 |
55 |
|
|
|
|
|
|
.510 |
Extraction Method: Principal Component Analysis; Rotation Method: Varimax with Kaiser Normalization; Note: (Values<.4 are suppressed).
Seven factors extracted by factor analysis and according to diagnostic manual seven symptoms required to identify this behavioural disruption. Some factors explained single symptom but few others muddled with each other, expressing some symptoms in an alternate feature or domain. For example, two symptoms deceitfulness and aggressiveness fall in a single domain. Contrary a single symptom impulsivity and non-consideration scattered into two aspects. Similarly, lack of remorse or compensation is a single symptom but segregated into two dimensions. Exploratory factor analysis explored 7 factors which explained 62.35% variance. Factors with one item were rejected and seven factors left. Items with factor loading below .4 were eliminated, and factor loading of this scale ranged from .44 to .72 (Table II).
Confirmatory factor analysis (CFA): Amos Graphics7 was used to run the confirmatory factor analysis. Outcomes that drawn though EFA drained conclusions were accepted through CFA. Finalizing the same seven extracted factors with just reduction of items, bottommost two and uppermost eight questions in an aspect.
Although CMIN/DF and RMSEA values were acceptable but to improve the model doubtful questions of modification indices; covariance and regression weight were detected and discarded.
Table IV: Model fit summary of confirmatory factor analysis (n=234)
|
P Value |
CMIN/DF |
GFI |
AGFI |
CFI |
RMSEA |
RMR |
|
.000 |
1.914 |
.838 |
.798 |
.917 |
.063 |
.043 |
CMIN/DF: chi-square minimum/degree of freedom; GFI: Goodness of Fit Index; CFI: Comparative Fit Index, AGFI: Adjusted Goodness of Fit Index; RMSEA: Root Mean Square of Error Approximation
Figures of confirmatory factor analysis of ASPDS of adults having 7 factors depicted in the above-mentioned table. The above figure got through the deletion of unconvinced queries i.e., 1, 2, 4, 8, 11, 14, 17, 18, 20, 22, 23, 24, 26, 28, 31, 34, 35, 37, 38, 40, 41, 43, 44, 45, 46, 47, 49, 52, 54, 55, 56, 57, 60, 61, 62, 64, 65, and 66. Model fit indicated CFI = .917, GFI = .838, RMSEA = .063, and CMIN/DF = 1.91, with significance level p< .001. the resultant values depicted the appropriateness of the measure.
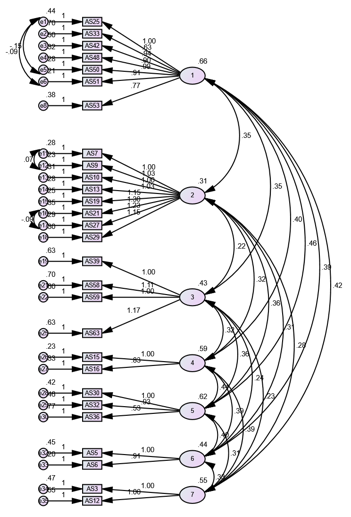
Figure 1: Confirmatory factor analysis of Antisocial Personality Disorder Scale
Confirmatory factor analysis resulted in 28 Antisocial Paranoid Personality Disorder Scale for Adults.
Confirmatory factor analysis resulted in 28 Antisocial Paranoid Personality Disorder Scale for Adults.Phase II: Determination of Psychometric Properties of Antisocial Personality Disorder Scale
a) Cronbach’s Alpha Reliability: Cronbach Alpha of Antisocial Personality Disorder Scale presented in the Table.
Table V: Cronbach alpha of Antisocial personality disorder scale (n=234)
|
Scale |
Cronbach’s Alpha |
Number of Items |
Sig |
|
|
Antisocial Personality Disorder Scale (ASPDS) |
.943 |
28 |
.000 |
|
|
Antisocial Personality Disorder has .94 Cronbach alpha reliability coefficient which is highly significant value and well supported by literature.
Table VI: Cronbach alpha of subscales of antisocial personality disorder scale (n=234) |
||||
|
Subscales |
Total items |
Cronbach Alpha |
|
1 Apathy |
7 |
.891 |
|
2 Deceitfulness and aggressiveness |
8 |
.911 |
|
3 Egocentric |
4 |
.753 |
|
4 Lack of remorse |
2 |
.768 |
|
5 Impulsiveness |
3 |
.670 |
|
6 Recklessness |
2 |
.713 |
|
7 non-compensation behaviour |
2 |
.679 |
Note:**P<.01
The reliability of subscale ultimately contributed to the overall reliability of the whole scale and the subscales of antisocial personality disorder expressed a good reliability which is mentioned in table VI i.e., .891 of Apathy, .911 of deceitfulness and aggressiveness, .753 of egocentric, .768 of lack of remorse, .670 of impulsiveness, .713 of recklessness and .679 of non-compulsive behaviour.Construct validity of antisocial personality disorders scale : Sample of 55 (n=55) Male=32, Female=23 recruited from colleges and university faculty and students and community population.
i) Instrument: To validate Antisocial Personality Disorder Scale, translated version of SD3 (Short measure of Dark Triads); 12,13 subscale Psychopathy was picked. SD3, psychopathy was designed to assess the impulsivity, callousness, and antisocial behavior.
ii) Results
Table VII: Validity analysis of Antisocial personality disorder (n=55)
|
Scales |
1 |
2 |
|
1. AS |
- |
|
|
2. SD3* |
.692** |
- |
* Short measure of Dark Triad **p<.01
Convergent validity of ASPDS and SD3 Scale
was r = .692** which showed a moderate level reliability. SD3 scale consists of
27-items and it is used to measure the three traits of Machiavellianism,
narcissism, and psychopathy. These traits are related to the ASPDS.
ASPDS (English & Urdu versions) are given as Annexures (1 & 2). DISCUSSION The current study aimed to develop and evaluate the
psychometric properties of ASPDS for adults in the Urdu language. The findings
indicate that the ASPDS is a reliable and valid tool for assessing antisocial
personality traits, as evidenced by strong psychometric properties. EFA
identified a robust seven-factor structure, explaining 62.35% of the total
variance, while CFA validated the model with satisfactory fit indices (CFI =
0.917, RMSEA = 0.063). The final 28-item scale demonstrated excellent internal consistency
(Cronbach’s alpha = 0.94) and significant convergent validity, as reflected in
a strong positive correlation with the psychopathy subscale of the Short
Measure of Dark Triads (r = 0.692, p <0.01). These results highlight the
ASPDS as a comprehensive, psychometrically sound instrument for assessing
antisocial personality disorder in Urdu-speaking populations, fulfilling the
study’s primary objective. ASPDS analysis
determines seven facets, removing below .4 value item that were 4 in number,
revealing 60.22% variance and .40 to .73 factor loading. Furthermore,
Kaiser-Meyer-Olkin measure .93 was adequate, and Bartlett’s test of sphericity
was significant (p < .001). CFA finalized the same seven dimensions
as cited in DSM-V symptomatology, after modification, deletion and rejection of
items. After deleting 34 odd questions with high regression weights, proceed to
covariance check and following covariance has been executed between item 25 and
50, 25 and 51, 7 and 9, and 21 and 27 to enhance the values. Among 66 items 28
items were considered as the final supporting values scale. Model fit indicated
CFI = .917, GFI = .838, RMSEA = .063, and CMIN/DF = 1.91, with significance
level p < .001. Typically, values above 0.90 are regarded as
good but, values above 0.80 may be deemed acceptable. Simulation studies imply
that GFI and AGFI are dependent on sample size. Both indicators decrease with
increasing model complexity, especially for smaller sample sizes.14 Validity of antisocial personality scale
with Short Dark Triad subscale Psychopathy (SD3)12 translated into
Urdu language13 was moderate in range r = .692**. Rule of
thumb for Interpreting the Size of a Correlation Coefficient is .90 to 1.00 =
Very high positive correlation, .70 to .90 = High positive correlation, .50 to
.70 = Moderate positive correlation, .30 to .50 = Low positive correlation,
same rule for negative correlation. Reliability of scale and subscale was
excellent α = .943.15
All potential measurement models for the ASPDS have adequate fit indices, with only minor
variations between them. Because there aren't many screening tools
available for the diagnosis of antisocial personality disorder, a useful
and socially and culturally valid one was much needed. Since it's well-known
that tools created for one group of people may not be regarded as reliable and
consistent by other groups, it's better to have a tool with cultural criteria
than one without. This study filled the gap left by the paucity of research on
the antisocial personality scale in Pakistan by developing an important tool to
assess antisocial personality disorder.
Limitations of the study and suggestions The study has several methodological limitations. One
key limitation is the relatively small sample size, which may restrict the
generalizability of the findings. Future research should address this by
utilizing larger, more diverse samples from various linguistic and cultural
contexts to enhance the scale's applicability and robustness. Additionally,
further validation studies are recommended to strengthen the psychometric
soundness of the ASPDS. Adapting and translating the scale into other languages
would also enable its broader use across different populations. To establish criterion validity more comprehensively,
future studies should explore the scale's relationship with other validated
measures of antisocial behavior and attitudes. If the ASPDS demonstrates strong
alignment with antisocial behavior, particularly in forensic and correctional
settings, it could become a time-efficient tool for assessing such traits.
Expanding the scope of research to community-based samples and diverse contexts
where antisocial behavior can be measured would provide valuable insights and
further confirm the utility of the scale.
CONCLUSION
The
ASPDS is a psychometrically robust and culturally relevant tool for assessing
antisocial personality disorder in Urdu-speaking adults. Its strong
reliability, validity, and alignment with established measures underscore its
utility in both clinical and research settings. This 28-item scale provides
mental health professionals, researchers, and practitioners with a reliable
method to evaluate antisocial personality traits, making it particularly useful
in forensic, correctional, and community-based contexts. Additionally, the
ASPDS holds promise for monitoring the effectiveness of intervention programs
aimed at addressing criminal and antisocial behaviors. Future studies should
focus on further validation across diverse populations and contexts to expand its
applicability and ensure its broader use. REFERENCES 1. American Psychiatric Association. Diagnostic
Statistical Manual for Mental Disorders. (5th ed. TR). American
Psychiatric Publications; Arlington, VA, USA. 2013. ISBN: 978-0890425763. https://doi.org/10.1176/appi.books.9780890425787 2. Hashmani T, Jonason PK. Antisocial behavior. In:
Shackelford TK, Weekes-Shackelford VA, (eds). Encyclopedia of evolutionary
psychological science. Springer International Publishing; New York, NY, USA:
2017. pp. 1-6. 3. dos Santos W, Holanda L, Meneses G, Luengo MA,
Gómez-Fraguela JA. Antisocial behaviour: a unidimensional or multidimensional
construct? Avances en Psicología Latinoamericana 2019;37(1):13-27. https://doi.org/10.12804/revistas.urosario.edu.co/apl/a.5105 4. de Farias MSJA, Gomes ARF, Calheiros MB, Cavalcante HPA,
Lessa MM, Neto VLM. The antisocial personality disorder and its
characteristics, changes and advances: a challenge. Int J Collab Res Intern Med
Public Health 2013;100(2):95-102. 5. Dean K, Korobanova D. Antisocial personality disorder
managing the healthcare relationship. Med Today 2015;16(8):14-8. 6. Pemment J. Psychopathy versus sociopathy: why the
distinction has become crucial. Aggress Violent Behav 2013;18(5):458-61. 7. Black DW. The natural history of antisocial personality
disorder. Can J Psychiatry 2015;60(7):309-14. https://doi.org/10.1177/070674371506000703 8. Del-Ben CM. Neurobiology of personality disorder antisocial.
J Clin Psychiatry 2005;32(1):27-36. https://doi.org/10.1590/S0101-60832005000100004 9. Blackburn R, Fawcett DJ. The antisocial personality
questionnaire: an inventory for assessing deviant traits in offender
populations. Eur J Psychol Assess 1999;15(1):14-24. https://psycnet.apa.org/doi/10.1027/1015-5759.15.1.14 10. Hare RD. A research scale for the assessment of
psychopathy in criminal populations. Pers Individ Dif 1980;1(2):111-19. http://dx.doi.org/10.1016/0191-8869(80)90028-8 11. Tay L, Jebb A. Scale Development. In: Rogelberg SG
(editor), The SAGE Encyclopaedia of Industrial and Organizational Psychology.
2nd ed. 2017. SAGE Publications, New Delhi, India. https://doi.org/10.4135/9781483386874 12. Jones DN, Paulhus DL. Introducing the Short Dark Triad
(SD3): a brief measure of dark personality trait. Assessment 2013;21(1):28–41. https://doi.org/10.1177/1073191113514105 13. Gul-e-Sehar, Fatima I. Dark triad personality traits as
predictors of bullying and victimization in adolescents. J Behav Sci
2016;26(1):51-65. 14. Mulaik SA, James LR, Van Alstine J, Bennett N, Lind S,
Stilwell CD. Evaluation of goodness-of-fit indices for structural equation
models. Psycholo Bull 1989;105(3):430–45. https://psycnet.apa.org/doi/10.1037/0033-2909.105.3.430 15. Hinkle DE, Wiersma W, Jurs SG. Applied Statistics for the
Behavioral Sciences (5th ed). Houghton Mifflin, Boston, Mass,
London, UK. 2003. Following authors have made substantial contributions to the
manuscript as under: SR
& ZB: Conception and study design,
acquisition, analysis and interpretation of data, drafting the manuscript,
critical review, approval of the final version to be published Authors agree to be
accountable for all aspects of the work in ensuring that questions related to
the accuracy or integrity of any part of the work are appropriately
investigated and resolved.
CONFLICT OF INTEREST Authors
declared no conflict of interest, whether financial or otherwise, that could
influence the integrity, objectivity, or validity of
their research work.
GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors
declared no specific grant for this research from any funding agency in the
public, commercial or non-profit sectors
DATA SHARING STATEMENT The data that support the findings of this
study are available from the corresponding author upon reasonable request
KMUJ
web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk
APPENDIX-01 Antisocial
Personality Disorder Scale Test
Instructions Item
Scoring Format 1 = Strongly
Disagree. 2 = Disagree. 3 = To some extent. 4 = Agree. 5 = Strongly
Agree. *No reverse
scoring for any item. Subscales Item No. Total items 1. Apathy 1-7 7 2. Deceitfulness and aggressiveness 8-15 8 3. Egocentric 16-19 4 4. Lack of remorse 20-21 2 5. Impulsiveness 22-24 3 6. Recklessness 25-26 2 7. Non-compensation behaviour 27-28 2
APPENDIX-02
![]() This
is an Open Access article distributed under the terms of the Creative
Commons Attribution 4.0 International License.
This
is an Open Access article distributed under the terms of the Creative
Commons Attribution 4.0 International License.