![]() https://doi.org/10.35845/kmuj.2025.23317 ORIGINAL ARTICLE
https://doi.org/10.35845/kmuj.2025.23317 ORIGINAL ARTICLE
Development and validation of an indigenous Urdu measure for Schizoid personality disorder in adults
Samia Rasheed ![]() 1,2, Zaqia
Bano
1,2, Zaqia
Bano ![]() 2, 3
2, 3
|
1: Department of Psychology, University of Gujrat, Gujrat, Pakistan 2: Department of Psychology, National University of Medical Sciences, Rawalpindi, Pakistan 3: Department of Clinical Psychology, NUR International University, Lahore, Pakistan
Email
Contact #: +92-347- 6681017
Date Submitted: February 07, 2023 Date Revised: June 16, 2024 Date Accepted: July 03, 2024 |
|
THIS ARTICLE MAY BE CITED AS: Rasheed S, Bano Z. Development and validation of an indigenous Urdu measure for Schizoid personality disorder in adults. Khyber Med Univ J 2025;17(Suppl 1):S12-S19. https://doi.org/10.35845/kmuj.2025.23317 |
ABSTRACT
Objective: To develop and validate an indigenous Urdu scale for assessing schizoid personality disorder in adults and to evaluate its psychometric properties.
Methods: This cross-sectional study, conducted between February and June 2019, utilized Diagnostic and Statistical Manual of Mental Disorders-5 criteria, existing literature, and clinical observations to develop a 63-item pool. After expert review and pilot testing, a 43-item scale was administered to 234 participants (123 males, 111 females) aged 18 to 60 years, drawn from both clinical and non-clinical populations in Gujrat, Pakistan. The scale underwent exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) to refine the items, resulting in a 14-item measure with three subscales: solitariness, emotional coldness, and indifference to praise. The psychometric properties, including reliability and convergent validity, were assessed using Cronbach's alpha and the University of California, Los Angeles (UCLA) Loneliness Scale (Version 3).
Results: The Indigenous Schizoid Personality Disorder Scale (SPDS) exhibited robust psychometric properties. EFA identified four factors, with three confirmed through CFA. The scale demonstrated excellent model fit indices (CMIN/DF=1.765, CFI=0.955, RMSEA=0.057). Cronbach's alpha for the total scale was 0.887, with subscale reliabilities ranging from 0.768 to 0.852. Convergent validity was supported by a significant positive correlation (r = 0.452, p<0.01) with the UCLA Loneliness Scale.
Conclusion: The 14-item Indigenous SPDS demonstrated strong psychometric properties, providing a culturally relevant and reliable tool for assessing schizoid personality disorder in Urdu-speaking populations. This scale holds significant value for researchers, clinical psychologists, students, and mental health practitioners, enhancing its utility across diverse clinical and non-clinical settings.
Keywords: Schizoid Personality Disorder (MeSH); Scale development(Non-MeSH); Convergent validity (Non-MeSH); Reliability(Non-MeSH).
INTRODUCTION
Schizoid personality disorder is characterized by a pervasive pattern of social interaction disengagement and a limited emotional expressive repertoire in interpersonal contexts. People who suffer from schizoid personality disorder tend to withdraw from society significantly, and others may perceive them as strange, reclusive, or alone. Individuals suffering with schizoid personality disorder find it extremely difficult to engage with others, and they utilize introversion as a coping strategy to prevent emotional distress. Originally, the term "schizoid" was used to characterize the prodromal seclusion and lonesomeness associated with schizophrenia.1
Inability to experience joy, pleasurable phases of life and moods that other experience is termed as schizoid disorder. There are two discrete categories of patients with schizoid personality disorder: one who are shy, inept, isolated and fearful but appreciates sociability, other there are asocial, eccentric, persons who wants to be alone and have trouble in maintaining relationships with others even peers, resulting in scapegoating.2
Schizoid personality disorder has a complicated etiology that includes psychological, environmental, and hereditary components. Studies on the etiology of schizoid personality disorder are scarce. Nonetheless, research on personality disorders in general as well as the etiology of cluster A personality disorders are ongoing. Personality disorders have a complicated and multifaceted etiology. Numerous biological variables influence how a person's personality develops. A fundamental psychobiological trait that is inherited, temperament plays a major role in the formation of personality.3 Epigenetic pathways, which include life experiences like trauma and socioeconomic circumstances, further affect temperament. In personality development, these are known as adaptive etiological factors.4
Compared to other adult personality disorders, children with major depressive disorder who also acquire a personality disorder are more likely to develop schizoid, avoidant, borderline, or schizotypal personality disorders. Additionally, the likelihood of schizoid personality features was higher in adult convicts who had been incarcerated as children.5
Schizoid personality disorder is mostly occurred in males.6 National Comorbidity Survey Replication proposed 4.9% prevalence but it is not common in clinical setting Diagnostic and Statistical Manual of Mental Disorders- 5 (DSM-5).7 According to a study about 1% from general population and 2% from clinical population were diagnosed as a schizoid and most of them were adolescents or young adults, may be due to parental or school pressure. Its onset is usually in childhood, chronic in childhood. It remains stable through adolescents and adulthood as well and may convert to schizotypal and schizophrenia.8
In psychiatry and psychology, personality disorders are a common topic of discussion. However, without an understanding of the typical course of personality development, we are unable to comprehend dysfunction or abnormality. While personality has long been a topic of interest for researchers, psychologists, therapists, psychoanalysts, and psychiatrists. The majority of psychological tests used in Pakistan and other nations are written in English. It is being overlooked that cultural variations could taint the answer, which is a very significant element. The usage of standardized examinations across cultural boundaries has raised some problems, making cross-cultural assessment a delicate topic. Given that culture affects many facets of a person's life, it is likely to have an impact on how psychological constructs are measured.
The current study's goal was to create and validate an adult schizoid personality disorder scale in the Urdu language.
For ethical concerns, the Departmental Research Review Committee (DRRC) of the
Psychology Department at the University of Gujrat, Pakistan, accepted the
study. It was carried out between February 15 and June 20, 2019. Data for the
study was gathered from several government and private colleges, universities,
hospitals, and communities in Gujrat, Pakistan, using a cross-sectional
analytical study methodology.
The development of a schizoid personality disorder scale served as the foundation for the first phase of research. Standardized approaches for developing scales were employed in the development of the adult schizoid personality disorder scale.9 A pool of items was created to evaluate that specific condition. The items were generated using the ordinal level assessment and arranged sequentially from weaker to stronger phrases. Items were created using literature, diagnostic guidelines, and symptoms of schizoid personality disorder. Multiple choice questions were included in the questionnaire's design.
A total of 63 items were generated after deep study of schizoid personality disorder in the Diagnostic and Statistical Manual of Mental Disorders-fifth edition, existing available literature, and people's opinions using both the inductive and deductive approach. Further, these generated questions were evaluated by the panel of 5 PhD experts in expert evaluation meeting. Experts considered each item with respect to its essentiality, appropriateness of material with reference to adults and construct of obsessive-compulsive personality. After the vigilant analysis 43 items were finalized for tryout. Try out was implemented to check the user appropriateness and understanding about the test to identify potential problem. The test administered on 104 participants using Likert rating scale i.e., strongly disagree “1”, disagree “2”, to some extent “3”, agree “4” and strongly agree “5” and reverse scoring for reverse questions. These items served as symbols for the individual beliefs, deeds, and interpersonal relationships of every person. The final phase contained a sample of 234 subjects, (males = 123, females = 111) over the age of 18. They were chosen, with their permission, from a variety of educational environments, such as clinics, community centers, colleges, universities, and professional staff and pupils.
After receiving approval from the head of the relevant institution, the participant signed an informed consent form. The participants then completed the demographic form and questionnaire.
Inclusion criteria
I. Age range of participants were between 18 years to onward.
II. Participants were recruited from both clinical and non-clinical population.
III. Participants were drafted from community, educational institutes; government and private school teachers, college and university faculty and students, and health institutes; hospitals.
IV. Both males and females were included.
V. Cultural context was considered.
Exclusion criteria
I. Below 18 years population were excluded.
II. People with Physical disability were excluded.
III. People with psychotic disorder and intellectual disability were also excluded.
Sampling technique: Purposive sampling technique was employed to recruit the participants. Purposive sampling technique is a type of non-probability sampling technique which is based on characteristics of a population and the objective of the study.
Research instruments: The instruments which were used in this study are informed consent form, demographic form and indigenous Schizoid Personality Disorder Scale.
Ethical consideration: Ethical consideration like voluntary participation, informed consent, anonymity, confidentiality was maintained throughout the process of research.
Correlation analysis: Correlation analysis was run on the scale and below 0.4 values item were discarded. Afterward, a pilot study was done and the data of the pilot study investigated using item-total correlation of the questions. A sample of 104 adults with age range above 18 years were employed and 43 items scale was administered. Subsequently, a pilot study was done and the data of the pilot study investigated using item-total correlation of the questions. Questions were confirmed with correlation coefficients above 0.40 and remaining with lower values were discarded. These remaining items were reliable for final administration of the scale. For final administration 234 adults (Male= 123, Female= 111) from age above 18 years were included.
The data analyzed by using correlation, exploratory factor analysis, confirmatory factor analysis and reliability test using Statistical Package for Social Sciences (SPSS-21) and Analysis of a Moment Structures (AMOS-21).
RESULTS
The analysis revealed significant positive correlations (p < 0.01) for all 22 items of the Schizoid Personality Disorder Scale (Table 1). The factor loading values, ranging from 0.413 to 0.659, exceeded the established threshold of 0.40, confirming their appropriateness for assessing schizoid personality traits as supported by existing literature. 10
Table I: Correlation coefficient of 22 items of Schizoid personality disorder (n=10)
|
Sr. No. |
Item No. |
R |
Sr. No. |
Item No. |
R |
|
1 |
1 |
.516** |
12 |
23 |
.554** |
|
2 |
2 |
.611** |
13 |
25 |
.413** |
|
3 |
3 |
.427** |
14 |
30 |
.542** |
|
4 |
4 |
.550** |
15 |
35 |
.426** |
|
5 |
5 |
.554** |
16 |
37 |
.601** |
|
6 |
7 |
.417** |
17 |
38 |
.505** |
|
7 |
11 |
.457** |
18 |
39 |
.546** |
|
8 |
14 |
.659** |
19 |
40 |
.502** |
|
9 |
15 |
.551** |
20 |
41 |
.497** |
|
10 |
21 |
.477** |
21 |
42 |
.469** |
|
11 |
22 |
.443** |
22 |
43 |
.415** |
**. Correlation is significant at the 0.01 level (2-tailed) **
Exploratory factor analysis (EFA): The items with less than .4 values were suppressed. Factor loading find the relationship range between factor and item. Factor loading prescribed value is +1 to -1, the extent to which factor loading closer to +1 or -1, there will be higher association among factors. Significant cut-off value for factor loading is .32,11 but literature also supported .3 - .4.12
Table II shows the Kaiser-Meyer-Olkin measure of sampling adequacy i.e., .896 and significant Bartlett’s test of sphericity significant i.e., p<.001. Predominantly factors labelled with 58.89% variance. Items with factor loading below .4 were eliminated, and factor loading ranging from .49 to .77.
Table II: Kaiser-Meyer-Olkin (KMO) and Bartlett’s test of sphericity (n=234)
|
Variable |
KMO |
Bartlett’s Test |
||
|
Chi-Square |
Df |
Sig |
||
|
Schizoid Personality Disorder Scale (SPDS) |
.896 |
2502.238 |
231 |
.000 |
The factor analysis with varimax rotation identified four distinct factors, with factor loadings ranging from 0.497 to 0.761. Each item demonstrated strong alignment with its respective factor, confirming the scale's multidimensional structure for assessing schizoid personality traits (Table III).
Table III: Factor loading of 21 item on Schizoid personality disorder scale
after varimax rotation (n=234)
|
Sr. No. |
Item No. |
1 |
2 |
3 |
4 |
|
1 |
1 |
.674 |
|
|
|
|
2 |
3 |
.644 |
|
|
|
|
3 |
7 |
.748 |
|
|
|
|
4 |
15 |
.597 |
|
|
|
|
5 |
19 |
.761 |
|
|
|
|
6 |
20 |
.751 |
|
|
|
|
7 |
12 |
|
.578 |
|
|
|
8 |
14 |
|
.575 |
|
|
|
9 |
16 |
|
.739 |
|
|
|
10 |
17 |
|
.777 |
|
|
|
11 |
18 |
|
.497 |
|
|
|
12 |
21 |
|
.747 |
|
|
|
13 |
22 |
|
.745 |
|
|
|
14 |
2 |
|
|
.604 |
|
|
15 |
4 |
|
|
.529 |
|
|
16 |
5 |
|
|
.544 |
|
|
17 |
8 |
|
|
.574 |
|
|
18 |
9 |
|
|
.698 |
|
|
19 |
10 |
|
|
.745 |
|
|
20 |
11 |
|
|
.622 |
|
|
21 |
13 |
|
|
|
.723 |
Confirmatory
factor analysis (CFA): There was total four factors explored
through EFA, which was further run through CFA and final three factors were
confirmed with changing number of questions, minimum three and maximum six.
Model fit indices values of CMIN/DF and RMSEA were satisfactory but to better
fit the model CFI modification indices of covariance and regression weights
were applied. Problematic questions were observed in regression weight,
modification indices, and that Problematic items were discarded. Item deleted
until the good CFI value establishment.
The
confirmatory factor analysis revealed an excellent model fit, with key indices
meeting recommended thresholds (Table IV). These results support the validity
and robustness of the scale's factor structure.
Table IV: Model fit summary of confirmatory factor analysis (n=234)
|
P Value |
CMIN/DF |
GFI |
AGFI |
CFI |
RMSEA |
RMR |
|
.000 |
1.765 |
.927 |
.895 |
.955 |
.057 |
.069 |
CMIN/DF: chi-square minimum/degree of freedom; GFI: Goodness of Fit Index; CFI: Comparative Fit Index, AGFI: Adjusted Goodness of Fit Index; RMSEA: Root Mean Square of Error Approximation, RMR:root mean square residual
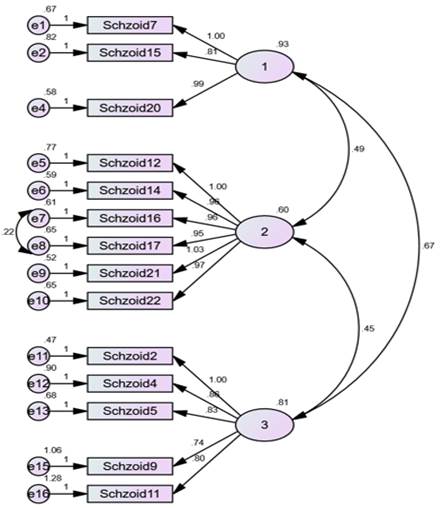
Figure 1: Confirmatory factor analysis of Schizoid Personality Disorder Scale
The confirmatory factor analysis (Figure 1) illustrates the three-factor structure of the Schizoid Personality Disorder Scale, confirming the relationship between the latent constructs (factors) and their observed variables (items). Each factor (labeled 1, 2, and 3) is linked to a subset of items with standardized regression weights, all exceeding the acceptable threshold.onfirmatory factor analysis ended in 14 item Schizoid Personality Disorder Scale for Adults.
Phase II: Determination of Psychometric Properties of Schizoid Personality Disorder Scale
Schizoid Personality Disorder Scale demonstrated strong internal consistency with a Cronbach's alpha of 0.887 (p < 0.01), confirming its reliability (Table V).
a) Cronbach’s alpha reliability: Schizoid Personality Disorder has very well (.88) Cronbach alpha reliability coefficient (Table V).
Table V: Cronbach alpha of Schizoid personality disorder scale (n=234)
|
Scale |
Cronbach’s Alpha |
Number of Items |
Sig |
|
Schizoid Personality Disorder Scale (SPDS) |
.887 |
14 |
.000 |
The subscales showed good reliability: Solitariness had an alpha of 0.775, Emotional Coldness had 0.852, and Indifference to Praise had 0.768. All values are within acceptable ranges for psychometric reliability (Table VI).
Table VI: Cronbach alpha of subscales of Schizoid personality disorder scale (n=234)
|
Subscales |
Total items |
Cronbach Alpha |
|
1. Solitariness |
3 |
.775 |
|
2. Emotional coldness |
6 |
.852 |
|
3. Indifferent to praise |
5 |
.768 |
Note: **P<.01
b) Construct validity of schizoid personality disorders scale: Sample of 54 (N=54) Male=27, Female=27 employed from colleges and university faculty and students and community population. To estimate the convergent validity of Schizoid Personality Disorder Scale two alike scale were used. UCLA Loneliness Scale (Version 3);13 measure aloofness, solitariness and disconnection to others.
The validity analysis revealed a significant positive correlation (r = 0.452, p < 0.01) between the Schizoid Personality Disorder Scale and the UCLA Loneliness Scale (Version 3), indicating acceptable convergent validity between the two measures (Table VII).
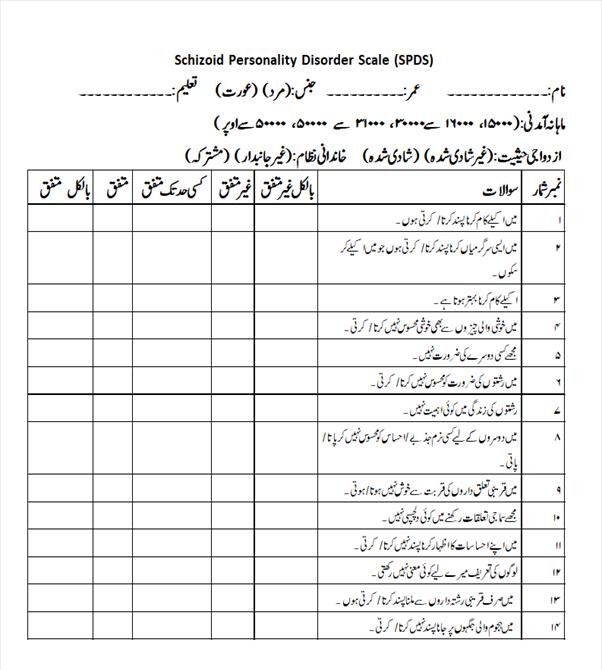
Schizoid Personality Disorder Scale (English & Urdu versions) are given as Annexures (1&2).
Table VII: Validity analysis of Schizoid personality disorder scale (n = 54)
|
Scales |
1 |
2 |
|
1. Schizoid |
- |
|
|
2. UCLA-R |
.452** |
- |
Note: ** p<.01; UCLA = loneliness Scale (Version 3)
DISCUSSION
Our study on development and validation of the indigenous Urdu scale for assessing Schizoid Personality Disorder in adults provided strong evidence for its validity and reliability. The scale demonstrated excellent internal consistency, with a Cronbach's alpha of 0.887, and the subscales showed reliable scores ranging from 0.768 to 0.852. Factor analysis confirmed a robust three-factor structure with satisfactory model fit indices, including CFI and RMSEA values. The scale also exhibited good convergent validity, with a significant positive correlation (r = 0.452, p < 0.01) with the UCLA Loneliness Scale, indicating its effectiveness in assessing schizoid personality traits.
A psychiatric condition known as schizoid personality disorder is characterized by a restricted range of emotional expression in interpersonal contexts and a detachment from social connections. Schizoid personality disorder is characterized by aloofness, bluntness, isolation, disengagement, and remoteness in its sufferers. Schizoid personality disorder has a complicated etiology that includes psychological, environmental, and hereditary components. Because schizoid personality disorder can negatively impact many facets of life, early intervention and multidisciplinary care are essential. The assessment and treatment of schizoid personality disorder are demonstrated in this activity, which also emphasizes the importance of the interdisciplinary team in providing patients with better care.14
Schizoid personality disorder analysis explores 4 factors in rotation component matrix. Factor loaded above .4 value and ranges from .49 to .77 and 58.89% variance, KMO = .89, 0.5 KMO value considered as suitable value.15 The factor analysis of the seven-criterion schizoid personality disorder scales resulted in the three criteria by merging the seven criteria, mentioned in DSM-5. The CFA established three factors with 14 items by cancelling 7 challenging items. With every deletion CFA run again until accepted value. CFI = .955 and RMSEA = .057, GFI = .927; ≥.90 reflected well fit,16 AGFI= .895 and CMIN is less than .2 which is acceptable. All values are in acceptable range that better fit the model. Reliability value of schizoid scale is α = .887. Hinkle, Wiersma, and Jurs17 presented rule of thumb for Interpreting the Size of a Correlation Coefficient is .90 to 1.00 = Very high positive correlation, .70 to .90 = High positive correlation, .50 to .70 = Moderate positive correlation, .30 to .50 = Low positive correlation, same rule for negative correlation. The test was validated with University of California, Los Angeles (UCLA) Version 3 Loneliness Scale.13 UCLA Version 3 Loneliness Scale was strongly correlated with NYU Loneliness Scale r = .65**. Convergent validity of Schizoid Personality Disorder Scale and UCLA Version 3 Loneliness was r = .452** that is acceptable.
A competent screening tool that is both socially and culturally valid was desperately needed because there aren't many screening tools accessible to diagnose schizoid personality disorder. It is well known that tools created for one demographic may not be universally accepted as reliable and consistent for other populations. Thus, a tool that includes cultural specifications is preferable to others. This study developed an important tool to assess schizoid personality disorder in order to address the gap left by the paucity of research on the schizoid personality scale in Pakistan.
Further validation research can be carried out to improve its psychometric soundness. In order to be utilized globally, it can also be modified and translated into different languages. To enhance its application in psychiatric settings, more data on clinical samples can be gathered.
CONCLUSION
The 14-item Indigenous Schizoid Personality Disorder Scale was developed In Urdu, the national language of Pakistan. Researchers, psychologists, psychiatrists, social workers, and other mental health professionals can use this reliable and efficient technique for schizoid personality assessment for research as well as diagnostic purpose.
REFERENCES
1. Loch AA. Schizophrenia, not a psychotic disorder: bleuler revisited. Front Psychiatry 2019;10:328. https://doi.org/10.3389/fpsyt.2019.00328
2. Millon T, Davis RD. Schizoid personality disorders: The asocial pattern. In, Millon T, Davis RD (eds), Disorders of personality DSM-IV TM and beyond. 1996. Wiley & Sons, New York, USA.
3. Sanchez-Roige S, Gray JC, MacKillop J, Chen CH, Palmer AA. The genetics of human personality. Genes Brain Behav 2018;17(3):e12439. https://doi.org/10.1111/gbb.12439
4. Gescher DM, Kahl KG, Hillemacher T, Frieling H, Kuhn J, Frodl T. Epigenetics in personality disorders: today's insights. Front Psychiatry 2018;9:579. https://doi.org/10.3389/fpsyt.2018.00579
5. Yang M, Ullrich S, Roberts A, Coid J. Childhood institutional care and personality disorder traits in adulthood: findings from the British national surveys of psychiatric morbidity. Am J Orthopsychiatry 2007;77(1):67-75. https://doi.org/10.1037/0002-9432.77.1.67
6. Beck AT, Freeman AT & Associates. Cognitive therapy of personality disorders. 2004. Guilford Press, New York, USA.
7. American Psychiatric Association. Diagnostic statistical manual for mental disorders. 5th ed. Arlington, V.A: American Psychiatric Publications; 2013.
8. Blagov P, Ortigo KM. Schizoid Personality Disorder and Gender. In, Nadal KL, The SAGE Encyclopaedia of Psychology and Gender. 2017:1442-4. SAGE Publications Inc, Thousand Oaks, California. https://doi.org/10.4135/9781483384269
9. Tay L, Jebb A. Scale Development. In: Rogelberg S, ed. The SAGE Encyclopaedia of Industrial and Organizational Psychology. 2nd ed. 2017. SAGE Publications Inc, Thousand Oaks, California.
10. Rahn M. Factor analysis: a short introduction, part 5–dropping unimportant variables from your analysis 2018. [Accessed on: July 20, 2019]. Available from URL: https://www.theanalysisfactor.com/fa ctor-analysis-5
11. Worthington RL, Whittaker TA. Scale development research: a content analysis and recommendations for best practices. Couns Psychol 2006;34(6):806-38. http://dx.doi.org/10.1177/0011000006288127
12. Miller-Carpenter S. Ten steps in scale development and reporting: a guide for researchers. Commun Methods Meas 2018;12(1):25-44. http://dx.doi.org/10.1080/19312458.2017.1396583
13. Russell DW. UCLA Loneliness Scale (Version 3): reliability, validity, and factor structure. J Pers Assess 1996;66(1):20-40. https://doi.org/10.1207/s15327752jpa6601_2
14. American Psychiatric Association. Diagnostic and statistical manual of mental disorders (5th ed., text rev.). 2022. Arlington, V.A: American Psychiatric Publications https://doi.org/10.1176/appi.books.9780890425787
15. Tabachnick BG, Fidell LS. Using multivariate statistics. 5th ed. 2007. 2007.: Pearson Education Inc. Boston, New York, USA.
16. Hooper D, Coughlan J, Mullen M. Structural equation modelling: guidelines for determining model fit. Electron J Bus Res Methods 2008;6(1):53-60.
17. Hinkle DE, Wiersma W, Jurs SG. Applied Statistics for the Behavioral Sciences. 5th ed. 2003. Houghton Mifflin, Boston.
|
Following authors have made substantial contributions to the manuscript as under:
SR & ZB: Conception and study design, acquisition, analysis and interpretation of data, drafting the manuscript, critical review, approval of the final version to be published
Authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST Authors declared no conflict of interest, whether financial or otherwise, that could influence the integrity, objectivity, or validity of their research work.
GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |
APPENDIX-01
Schizoid Personality Disorder Scale
Test Instructions
Item Scoring Format
1 = Strongly Disagree. 2 = Disagree. 3 = To some extent. 4 = Agree. 5 = Strongly Agree.
*No reverse scoring for any item.
|
Subscales |
Item No. |
Total items |
|
1. Solitariness |
1-3 |
3 |
|
2. Emotional coldness |
4-9 |
6 |
|
3. Indifferent to praise |
10-14 |
5 |
APPENDIX-02