![]() https://doi.org/10.35845/kmuj.2024.23294 ORIGINAL
ARTICLE
https://doi.org/10.35845/kmuj.2024.23294 ORIGINAL
ARTICLE
Comparative effects of kinesiotaping with and without combined chain exercises on pain, range of motion, and quality of life in knee osteoarthritis: a randomized control trial
Sobia Maqbool ![]() 1, Hina Gul
1, Hina Gul ![]() 1, Janisar Zainab
1, Janisar Zainab ![]() 1 , Rida Mustafa
1 , Rida Mustafa ![]() 2
2
|
1: Faculty of Rehabilitation and Allied Health Sciences, Riphah International University, Lahore, Pakistan 2: Department of Physical Therapy, Faculty of Allied Health Sciences, The Superior University, Lahore, Pakistan
Email Contact #: +92-321-4979172
Date Submitted: December 29, 2022 Date Revised: August 01, 2024 Date Accepted: October 26, 2024 |
|
THIS ARTICLE MAY BE CITED AS: Gul H, Maqbool S, Zainab J, Mustafa R. Comparative effects of kinesiotaping with and without combined chain exercises on pain, range of motion, and quality of life in knee osteoarthritis: a randomized control trial. Khyber Med Univ J 2024;16(4):328-33. https://doi.org/10.35845/kmuj.2024.23294 |
ABSTRACT
Objectives: To compare the effects of Kinesiotaping (KT) with and without Combined Chain Exercises (CCEs) on pain, range of motion (ROM), and quality of life in patients with knee osteoarthritis (OA).
Methods: This randomized control trial was conducted at Riphah Rehabilitation Center and Ittefaq Hospital, Lahore, over six months. Thirty-eight patients with Grade II knee OA (Kellgren and Lawrence classification) aged 40–60 years were recruited using a convenience sampling technique and allocated into two groups via the lottery method. Group A received KT with CCEs, while Group B received KT only. Pain, ROM, and quality of life were assessed using the Numeric Pain Rating Scale (NPRS), goniometer, and SF-36, respectively, at baseline and after 4 weeks. Baseline treatment included hot packs and ultrasound. Statistical analyses were performed using paired and independent t-tests.
Results: Data from 34 participants (17 per group) were analyzed. Group A (KT with CCEs) showed statistically significant improvements compared to Group B (KT only) across all parameters: NPRS (p = 0.017), knee flexion (p = 0.035), knee extension (p = 0.004), and SF-36 (p = 0.002). Within-group comparisons also revealed significant improvements in Group A across all outcomes (p < 0.001).
Conclusion: KT combined with chain exercises significantly improved pain, ROM, and quality of life in knee OA patients compared to KT alone. These findings suggest that integrating CCEs with KT may provide more effective rehabilitation for knee OA.
Clinical trial registration number: NCT05334524
Keywords: Exercises (MeSH); Knee Osteoarthritis (MeSH); Osteoarthritis, Knee (MeSH); patients (MeSH); Quality of Life (MeSH); Range of Motion (MeSH); Range of Motion, Articular (MeSH).
INTRODUCTION
Osteoarthritis (OA), also known as wear-and-tear arthritis, degenerative joint disease (DJD), or age-related arthritis, is one of the leading causes of disability in the US and around the world. Inflammation of the joints is referred to as arthritis.1 The growth of osteophytes causes pain, edema, and restricted joint movement, and this degenerative joint disease promotes the rubbing of bones against one another. The syndrome causes synovial inflammation, sclerosis, and cysts to develop.2 Exercise therapy for knee OA improves cartilage metabolism and has an effect on cartilaginous structures via a mechanotransduction response.3 Stretching, open kinetic chain exercises (OKCE), and close kinetic chain exercises (CKCEs) were among the exercise treatment techniques taught.4 Kinesiotaping (KT) of the knee is used to relieve pain, improve active range of motion(AROM), and improve proprioception by correcting patella femoral alignment and reducing mechanical stress on the soft tissues.3
In the world, 18.0 percent of women and 9.6 percent of men over 60 show symptoms, making women more susceptible to the condition than males. Knee OA was diagnosed in 3.6% of participants in rural Pakistan and 3.1% to 4.6% of respondents in urban Pakistan.2 In February 2020, Nayanti AP, et al., released a double-blind randomized controlled trial to examine the impact of KT and strengthening of quadriceps muscle strength and functional status in women with knee osteoarthritis. The treatment and control groups had significantly different quadriceps muscular strength at the sixth week, but there were no significant differences present in the strengthening of quadriceps muscle at the fourth or eighth weeks or in Western Ontario and McMaster Universities Arthritis Index (WOMAC) values at the sixth week.5 Ye W, et al., conducted a systematic evaluation of eleven papers in 2020. In 490 people with OA of knee, the effectiveness of elastic taping on primary outcomes of pain and physical function, as well as secondary variables range of motion and muscular strength, were studied. There was a prominent improvement in pain, physical function, ROM (p=0.04), and strength of the quadriceps muscle with elastic taping, but no significant change in hamstring muscle strength.6
This research was conducted to identify a better therapy method for patients suffering from knee OA. This study will aid patients in changing their lifestyles and improving their quality of life by reducing pain and increasing range of motion, as well as improving functional capacities. This study will also help clinicians to apply better treatment protocol to knee OA patients to recover them from disability. Due to the lack of interest among patients about the clinical importance of KT and its applicability there is still a requirement for current evidence from systematic better-quality research. To the best of the researchers' knowledge, there is very little evidence available on the comparative effects of KT and combined chain exercises. Now this study looks into the comparative effects of only KT and combined chain exercises with kinesiotaping (CCEs + KT) in order to determine the most effective physical therapy approach for patients with knee OA.
METHODS
This randomized control trial was conducted at Riphah Rehabilitation Center and Ittefaq Hospital, Lahore, over six months following the approval of the study synopsis. A sample size of 38 was calculated using the EPITOOL sample size calculator based on SF-36 scores from a previous study.7
Participants were recruited using a convenience sampling method and randomized into two groups through the lottery method. Group A received Kinesio Taping combined with chain exercises (KT + CCEs), while Group B received Kinesio Taping (KT) alone. Patients were evaluated for pain (using the Numeric Pain Rating Scale, NPRS), range of motion (ROM, using a goniometer), and quality of life (using the SF-36 questionnaire) at baseline and after four weeks of treatment.
Inclusion and exclusion criteria: Participants aged 40–60 years with Grade II knee osteoarthritis based on the Kellgren and Lawrence classification were included.8 Patients with skin irritation, allergic reactions to tape, a history of knee injections or surgery, chronic illnesses (e.g., renal disease), or those using additional treatment protocols were excluded.3 Participants were instructed to maintain their regular activities and avoid other treatment modalities during the study.
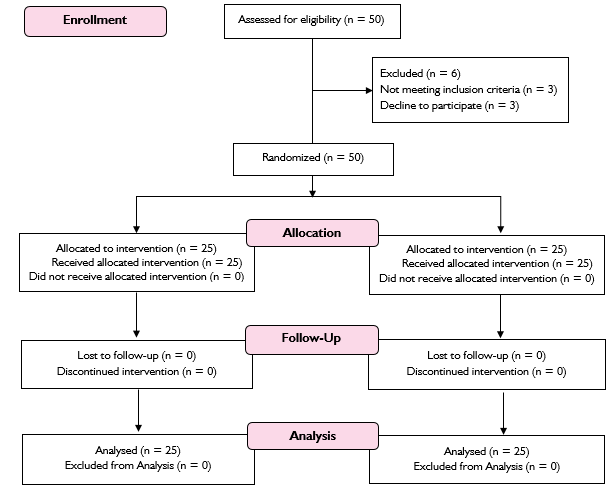
Figure 1: Methodology flow diagram of the study
Baseline treatment: All participants received conventional baseline treatment, including a heating pad for 10 minutes and continuous-mode ultrasound for 8 minutes.
Interventions
- Group A (KT + CCEs): Participants received Kinesio Taping along with combined chain exercises. Exercises included quadriceps setting, straight leg raises, full arc extensions, cycling in the air, wall slides, step-up and step-down exercises, lunges, and double-leg squats with isometric hip adduction. Each exercise consisted of 10 repetitions with 10-second holds.
- Group B (KT): Participants received KT only, using two "Y-strips" (20 cm each with a 2 cm anchor) and one "I-strip." The Y-strips were applied medially and laterally around the patella with 25% tension, and the I-strip was applied with 75% tension for 72 hours.
Each patient received two treatment sessions per week for four weeks.
Statistical analysis: Data from 34 participants (17 in each group) were included in the analysis after two dropouts per group. Normality was tested using the Shapiro-Wilk test. A paired t-test was used to compare outcomes between groups, while an independent t-test was applied to assess differences within groups. Statistical significance was set at p = 0.05.
RESULTS
The study included 34 participants after two dropouts in each group, with 17 participants in the KT + CCEs group and 17 in the KT group. The mean age of participants in the KT + CCEs group was 51.29 ± 6.48 years, while the KT group had a mean age of 48.00 ± 6.54 years. Mean BMI was comparable between groups, with 25.94 ± 2.61 in the KT + CCEs group and 26.12 ± 2.39 in the KT group. Gender distribution included 7 females and 10 males in the KT + CCEs group and 8 females and 9 males in the KT group.
Pain scores (NPRS) significantly improved post-treatment, with the KT + CCEs group reducing pain from a median of 7 to 3, compared to 5 in the KT group (p = 0.017) [Table I]. Knee flexion also improved significantly, increasing from 111.12 ± 7.55 to 126.06 ± 7.64 in the KT + CCEs group, compared to 120.00 ± 6.86 in the KT group (p = 0.035) [Table II]. Similarly, knee extension deficits improved significantly, with the KT + CCEs group reducing from 11.47 ± 3.79 to 3.40 ± 2.62, compared to 7.94 ± 4.87 in the KT group (p = 0.004) [Table III]. Quality of life (SF-36) scores also showed a significant post-treatment improvement, increasing from 46.9 to 57.3 in the KT + CCEs group, compared to 53.0 in the KT group (p = 0.002) [Table IV].
Table I: Comparison of pain score between the groups
|
Treatment |
Groups |
Median(IQR) |
p-value |
|
Pre-Treatment |
Kinesiotaping with combined chain exercises |
7(3) |
.936 |
|
Kinesiotaping |
7(3) |
||
|
Kinesiotaping with combined chain exercises |
3(3) |
.017 |
|
|
Kinesiotaping |
5(3) |
Table II: Pre and post comparison of knee flexion score
|
Treatment |
Groups |
Mean± SD |
Mean Difference |
t-statistic |
p-value |
|
Pre-Treatment |
Kinesiotaping with combined chain exercises |
111.1176±7.54886 |
.17647±2.28382 |
.077 |
.173 |
|
Kinesiotaping |
110.9412±5.62884 |
||||
|
Kinesiotaping with combined chain exercises |
126.0588±7.64420 |
6.05882±2.49038 |
2.433 |
.035 |
|
|
Kinesiotaping |
120.0000±6.85565 |
Table III: Pre and post comparison of knee extension scores
|
Treatment |
Groups |
Mean± SD |
Mean Difference |
t-statistic |
p-value |
|
Pre-Treatment |
Kinesiotaping with combined chain exercises |
11.47±3.79 |
-2.53±1.53 |
-1.65 |
.072 |
|
Kinesiotaping |
14.00±5.03 |
||||
|
Kinesiotaping with combined chain exercises |
3.40±2.62 |
-4.47±1.34 |
-3.32 |
.004 |
|
|
Kinesiotaping |
7.94±4.87 |
Table IV: Comparison of SF-36 quality of life score
|
Treatment |
Groups |
Median(IQR) |
p-value |
|
Pre-Treatment |
Kinesiotaping with combined chain exercises |
46.9(3.7) |
.735 |
|
Kinesiotaping |
46.7(3) |
||
|
Kinesiotaping with combined chain exercises |
57.3(4.9) |
.002 |
|
|
Kinesiotaping |
53(4.6) |
Within-group analysis (Table V) further confirmed significant improvements in the KT + CCEs group for all outcomes: pain reduced from 7.00 ± 1.45 to 3.41 ± 1.70, knee flexion increased from 111.12 ± 7.54 to 126.05 ± 7.64, knee extension improved from 11.47 ± 3.79 to 3.47 ± 2.62, and SF-36 scores rose from 47.17 ± 2.25 to 57.78 ± 3.32 (p < 0.001). The KT group also showed improvements, but less pronounced, with pain decreasing from 6.88 ± 1.41 to 4.88 ± 1.45, knee flexion increasing from 110.94 ± 5.63 to 120.00 ± 6.86, knee extension improving from 14.00 ± 5.03 to 7.94 ± 4.87, and SF-36 scores rising from 46.85 ± 2.10 to 53.04 ± 2.66 (p < 0.05).
Overall, the KT + CCEs group demonstrated superior outcomes in pain reduction, ROM improvement, and enhanced quality of life compared to the KT group alone.
Table V: Within group pain, quality of life and SF36 pre-post comparison
|
Tools |
Group A |
t-values |
p-values |
Group B |
t- values |
p- values |
||
|
Pre- Treatment |
Post- Treatment |
Pre-Treatment |
Post- Treatment |
|||||
|
Mean ± S.D |
Mean ± S.D |
Mean ± S.D |
Mean ± S.D |
|||||
|
NPRS |
7.00±1.45 |
3.41±1.698 |
29.16 |
.000 |
6.88±1.41 |
4.88±1.45 |
10.431 |
.000 |
|
Knee Flexion |
111.12±7.54 |
126.05±7.64 |
-9.42 |
.000 |
110.94±5.62 |
120.0±6.85 |
-5.829 |
.000 |
|
Knee Extension |
11.47±3.79 |
3.47±2.62 |
8.12 |
.000 |
14.00±5.03 |
7.94±4.87 |
3.43 |
.003 |
|
SF-36 |
47.17±2.25 |
57.78±3.32 |
-21.08 |
.000 |
46.85±2.10 |
53.04±2.66 |
- 8.52 |
.000 |
DISCUSSION
In this study, we investigated the efficacy of combining KT with CCEs in the treatment of knee OA. The findings revealed that time had a significant effect on all measured outcomes, including pain, range of motion (ROM), functional mobility, and quality of life, with a notable interaction between time and the intervention used. The study compared the effects of KT alone and KT combined with CCEs, demonstrating that the KT + CCEs group achieved significantly superior results across all parameters. Improvements in pain scores (NPRS), knee flexion and extension (ROM), and quality of life (SF-36) were significantly greater in the KT + CCEs group. Although both groups showed progress, the KT + CCEs group consistently outperformed the KT group, successfully addressing the study objective of identifying a more effective physical therapy intervention for knee OA management.
A study that produced similar results to the current study assessed the effectiveness of CCEs on pain, mobility, and physical function in people with knee OA. NPRS was used to assess pain, TUG was used to assess mobility, and lower extremity functional scale as used to assess physical function. Patients' pain was significantly reduced, and they were able to perform their ADLS with ease following treatment. CCEs with retro walking and perturbation exercises improved more. These findings appear to be consistent with the current study, which found improvements in pain, mobility, and physical function following conventional CKCEs that strengthened the knee joint. As in current study pain level decreased which assessed by NPRS and improved quality of life and improved ROM of knee flexion and extension in knee osteoarthritis patients by CCEs.9
A 2020 study by H, et al.,10 highlighted significant associations between knee pain and reduced function, range of motion, and quality of life. To evaluate the efficacy of Kinesio Taping in knee osteoarthritis treatment, the systematic review analyzed 18 randomized trials involving 876 patients. The review revealed significant improvements in VAS, WOMAC, and flexion ROM in KT groups compared to control groups, demonstrating that KT effectively reduces pain and enhances joint mobility in knee osteoarthritis patients. The systematic review discovered significant differences in VAS, WOMAC, and flexion range of motion between KT groups and control groups. KT improves performance. Based on prior findings, it is likely that an improvement in knee pain and function would also result in an increase in knee range of motion (ROM) and quality of life, as demonstrated in the current research. Even though prior research investigating the efficacy of KT as an adjuvant to exercise did not include ROM and quality of life as end variables, this study did. Previous research looked at the impact of KT as an exercise supplement. Furthermore, data from systematic studies shows that exercise programs are just as effective as KT programs in terms of boosting knee range of motion and quality of life.10
The study's goal was similar to the current study's goal, which was to evaluate the effects of KT for pain management in knee OA. This was a double-blind randomised controlled trial with 187 patients with knee OA divided into two groups. Group A was given KT, while Group B was the control group. For one month, Group A received KT on the knee. After 4 weeks of taping, pain was assessed at baseline. Pain was assessed using the Numeric Pain Rating Scale(NPRS) and Knee Injury and Osteoarthritis Outcome Score (KOOS). According to the findings, using tapes reduced pain, reduced the use of painkillers, and increased KOOS. After one month of treatment, the Kinesio Taping group had significantly reduced pain intensity.11 In present study, pain was measured through using NPRS, and there was lowering in pain and an increase in quality of life in the KT group, but there was a greater improvement in the KT with combine chain exercises group, which appears to support each other.
This finding is consistent with previous research published in 2017 by Taheri P, et al. They randomly assigned people to two study groups. Both groups received exercise therapy in addition to medications. Pain severity was assessed with a VAS and analgesic consumption was compared between two study groups before, three, and six weeks after treatment. There was no significant difference in pain severity (P = 0.228) or weekly analgesic consumption (P = 0.873) between the two groups at baseline. After three weeks, the taping group had significantly lower weekly analgesic consumption (P = 0.006) and pain intensity (P = 0.001) than the non-taping group. All outcomes were better for the group that received exercise and KT. Previous research backs up this conclusion. However, medication was also used as part of the rehabilitation program in previous studies. As a result, determining whether the improvement was purely due to the workouts and KT is quite difficult. Furthermore, Taheri and colleagues in 2017 concluded that there was no statistically significant difference in TUG scores between the two groups, which contradicts the findings of this study. Based on the results of this study, it seems that people with knee osteoarthritis can function better with a combination of treatments.12
In 2016, Olagbegi discovered that patients with knee osteoarthritis who took CCEs experienced significantly less knee pain and improved knee function. This conclusion is consistent with the study's findings, as both the patients' level of pain and their ability to function improved significantly after 8 weeks of treatment. The observed improvement in outcomes following CCEs could be attributed, at least in part, to an increase in quadriceps muscular strength. According to the study, strength training may activate the pain-relieving endorphin system by reducing the binding and availability of cerebral opioid receptors in key brain regions associated with reward and pain processing, positively modifying sensory input to the central nervous system and the gate control mechanism, and improving blood flow and cartilage nutrition, according to the research.13
Langendoen J, et al., compared the deformations that occurred when the tape was stretched by around 50% in 2016. They noticed that KT had a mechanical effect not only on the targeted tissues but also on the deeper layers, resulting in a variety of limb deformations. This was similar to the current study, which showed improvement in ranges by lengthening the soft-tissue layers of the knee.14
These boundaries can be seen in the thigh. The shearing of the epidermal and fascial layers changes when the tape is stretched in a specific direction, resulting in increased afferent stimulation. Castrogiovanni P, et al., discovered in 2016 that KT treatments that included tension worked better at reducing pain than those that did not.15
The similar findings shown by Pamuk and Yucesoy in 2015, as well as the reason why combining KT and CCEs had a greater impact in this study, could be attributed to the additional mechano stimulation effect caused by the KT application. This is the proposed reasoning taping over the skin is believed to stimulate cutaneous mechanoreceptors and enhance afferent signals to the central nervous system, resulting in pain relief. This idea has been shared. Pamuk and Yucesoy used magnetic resonance imaging in 2015 to show deformations in the entire limb after applying Kinesio tape to the skin, the tibialis anterior muscle, and the dorsal region of the foot with a fifty percent stretch.16
CONCLUSION
This study demonstrates that combining Kinesiotaping with Combined Chain Exercises is a more effective physical therapy approach for managing knee osteoarthritis compared to KT alone. The KT + CCEs group showed significantly greater improvements in pain reduction, range of motion (knee flexion and extension), and quality of life (SF-36 scores) than the KT group. These findings highlight the potential of incorporating CCEs into KT-based interventions to enhance treatment outcomes for patients with knee OA. Clinicians should consider integrating this combined approach into rehabilitation programs to optimize functional recovery, reduce disability, and improve overall patient quality of life. Further studies are recommended to explore the long-term benefits and applicability of this intervention in diverse patient populations.
REFERENCES
1. Lespasio MJ, Piuzzi NS, Husni ME, Muschler GF, Guarino A, Mont MA. Knee osteoarthritis: a primer. Perm J 2017;21:16-183. https://doi.org/10.7812/TPP/16-183
2. Badshah Y, Shabbir M, Hayat H, Fatima Z, Burki A, Khan S, et al. Genetic markers of osteoarthritis: early diagnosis in susceptible Pakistani population. J Orthop Surg Res 2021;16(1):124. https://doi.org/10.1186/s13018-021-02230-x
3. Danazumi MS, Ibrahim SU, Yakasai AM, Dermody G, Bello B, Kaka B. A comparison between the effect of combined chain exercises plus kinesio taping with combined chain exercises alone in knee osteoarthritis: a randomized clinical trial. Am J Phys Med Rehab 2021;100(11):1070-7. https://doi.org/10.1097/PHM.0000000000001705
4. Nahayatbin M, Ghasemi M, Rahimi A, Khademi-Kalantari K, Naimi SS, Tabatabaee SM, et al. The effects of routine physiotherapy alone and in combination with either tai chi or closed kinetic chain exercises on knee osteoarthritis: a comparative clinical trial study. Iran Red Crescent Med J 2018;20(4):1-8. https://doi.org/10.5812/ircmj.62600
5. Nayanti AP, Prabowo T, Sari DM. The effects of kinesio taping and quadriceps muscle strengthening exercise on quadriceps muscle strength and functional status in knee osteoarthritis. J Med Health 2020;2(5):40-50. https://doi.org/10.28932/jmh.v2i5.1555
6. Ye W, Jia C, Jiang J, Liang Q, He C. Effectiveness of elastic taping in patients with knee osteoarthritis: a systematic review and meta-analysis. Am J Phys Med Rehabil 2020;99(6):495-503. https://doi.org/10.1097/PHM.0000000000001361
7. Alburquerque-García A, Rodrigues-de-Souza DP, Fernández-de-las-Peñas C, Alburquerque-Sendín F. Association between muscle trigger points, ongoing pain, function, and sleep quality in elderly women with bilateral painful knee osteoarthritis. Journal of Manipulative and Physiological Therapeutics. 2015;38(4):262-8. https://doi.org/10.1016/j.jmpt.2014.10.018
8. Olagbegi OM, Adegoke BOA, Odole AC. Effectiveness of combined chain exercises on pain and function in patients with knee osteoarthritis. Bangladesh J Med Sci 2016;15(2):178-88. https://doi.org/10.3329/bjms.v15i2.24808
9. Koch M, Sarma PC, Dutta A, Kalita A. Effectiveness of combined kinetic chain exercises in the treatment of knee osteoarthritis in peri-menopausal and post-menopausal women in Guwahati, Assam, India. Int J Pharm Bio Sci 2022;12(1):38-46. https://doi.org/10.22376/ijpbs/lpr.2021.12.1.L38-46
10. Melese H, Alamer A, Temesgen MH, Nigussie F. Effectiveness of kinesio taping on the management of knee osteoarthritis: a systematic review of randomized controlled trials. J Pain Res 2020;13:1267. http://doi.org/10.2147/JPR.S249567
11. Donec V, Kubilius R. The effectiveness of Kinesio Taping® for pain management in knee osteoarthritis: a randomized, double-blind, controlled clinical trial. Ther Adv Musculoskelet Dis 2019;11:1759720X19869135. https://doi.org/10.1177/1759720X19869135
12. Taheri P, Vahdatpour B, Asl MM, Ramezanian H. Effects of taping on pain and functional outcome of patients with knee osteoarthritis: a pilot randomized single-blind clinical trial. Adv Biomed Res 2017;6:39. https://doi.org/10.4103/2277-9175.218031
13. Olagbegi OM, Adegoke BOA, Odole ACJ. Effectiveness of combined chain exercises on pain and function in patients with knee osteoarthritis. 2016;15(2):178-88. https://doi.org/10.3329/bjms.v15i2.24808
14. Langendoen J, Fleishman C, Kim SH, An HJ. Rationales and evidence of elastic taping: a clinician's perspective. J Int Acad Phys Ther Res 2016;7(1):979-88. http://dx.doi.org/10.20540/JIAPTR.2016.7.1.979
15. Castrogiovanni P, Di Giunta A, Guglielmino C, Roggio F, Romeo D, Fidone F, et al. The effects of exercise and kinesio tape on physical limitations in patients with knee osteoarthritis. J Funct Morphol Kinesiol 2016;1(4):355-68. https://doi.org/10.3390/jfmk1040355
16. Pamuk U, Yucesoy CA. MRI analyses show that kinesio taping affects much more than just the targeted superficial tissues and causes heterogeneous deformations within the whole limb. J Biomech 2015;48(16):4262-70. https://doi.org/10.1016/j.jbiomech.2015.10.036
AUTHORS' CONTRIBUTIONS Following authors have made substantial contributions to the manuscript as under: HG : Study design, acquisition of data, drafting the manuscript, critical review, approval of the final version to be published SM & JZ: Conception and study design, acquisition of data, drafting the manuscript, approval of the final version to be published RM: Analysis and interpretation of data, Drafting the manuscript, approval of the final version to be published
Authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST Authors declared no conflict of interest, whether financial or otherwise, that could influence the integrity, objectivity, or validity of their research work.
GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |