![]() https://doi.org/10.35845/kmuj.2023.23168 ORIGINAL
ARTICLE
https://doi.org/10.35845/kmuj.2023.23168 ORIGINAL
ARTICLE
Cone beam computed tomography evaluation of root canal morphology of maxillary premolars in North-West sub-population of Pakistan
Shahzad Ali Shah1,2
![]()
|
1: Department of Operative Dentistry, Khyber College of Dentistry, Peshawar, Pakistan 2: Department of Dental Repair, College of Dentistry, ArRass, Qassim University, Kingdom of Saudi Arabia
Email Date Submitted:October 02, 2022 Date Revised:February11, 2023 Date Accepted: May 11, 2023 |
|
THIS ARTICLE MAY BE CITED AS:Shah SA.Cone beam computed tomography evaluation of root canal morphology of maxillary premolars in North-West sub-populatıon of Pakistan. Khyber Med Univ J 2023;15(2):116-21. https://doi.org/10.35845/kmuj.2023.23168
|
ABSTRACT
OBJECTIVES: To determine the number and configuration of canals in permanent maxillary premolars using Cone Beam Computed Tomography (CBCT) and the relationship between canals count and patient gender in northwest region of Pakistan.
METHODS: This cross-sectional observational study was conducted at Khyber College of Dentistry (KCD) Peshawar, Pakistan. Data was collected from July 1st to 30th December 2020, using 133 patient’s CBCT scans with 266 maxillary premolar teeth. Roots and canals frequency as well as configurations were analyzed using Vertucci canal classification. CBCT images were obtained from Radiology department of KCD. Data were analyzed using SPSS-23 software,
RESULTS: Type-I Vertucci's canal composition was most common in first premolars (45.4%), followed by Type-IV (25.9%). Type-I was the most frequent find in second premolars (64.2%), followed by Type-III (15.4%). In Maxillary first premolars, 247 (92.8%) were single-rooted and 19 (7.14%) were two-rooted. In maxillary second premolars, 155(57.9%) were single-rooted, 110 (41.3%) were two-rooted, and one (0.37%) was three-rooted. In first & second premolar, single-root was the commonest root among males (92.7% & 58.4%) and females (30.8% and 19%) respectively. Gender-based difference in canal count in all premolars was not-significant. Mean tooth length of first and second premolar was 19.40±2.035 mm and 20.08±2.395 mm respectively. Mean crown length of first and second premolar was 6.05±0.752 mm and 5.69±0.505 mm respectively.
CONCLUSION: Most of the maxillary first and second premolars had Vertucci classification Type-I configuration. Gender-based diversity for number of canals was not-significant. All Vertucci canal configuration types were observed in maxillary premolars.
KEYWORDS: Maxillary Premolar (MeSH); Root Canal (MeSH); Cone Beam Computed Tomography (MeSH); Canal Configuration (MeSH); Khyber Pakhtunkhwa (Non-MeSH); Pakistan (MeSH)
INTRODUCTION
Anatomy of the root canals varies greatly in people of the same population and individuals of the same race.1 Therefore it is important to be aware of root canal variations, as this knowledge will help the clinicians to locate and treat previously unexplored canals during root canal treatment.2-4An accurate diagnosis that leads to accurate treatment is important for successful endodontic treatment and it relies on accurate interpretation of radiographic data.5Failure to negotiate all the canals, followed by a three-dimensional hermetic seal, can lead to unsuccessful endodontic treatment resulting in persistent periapical microorganisms and necrotic tissue.6
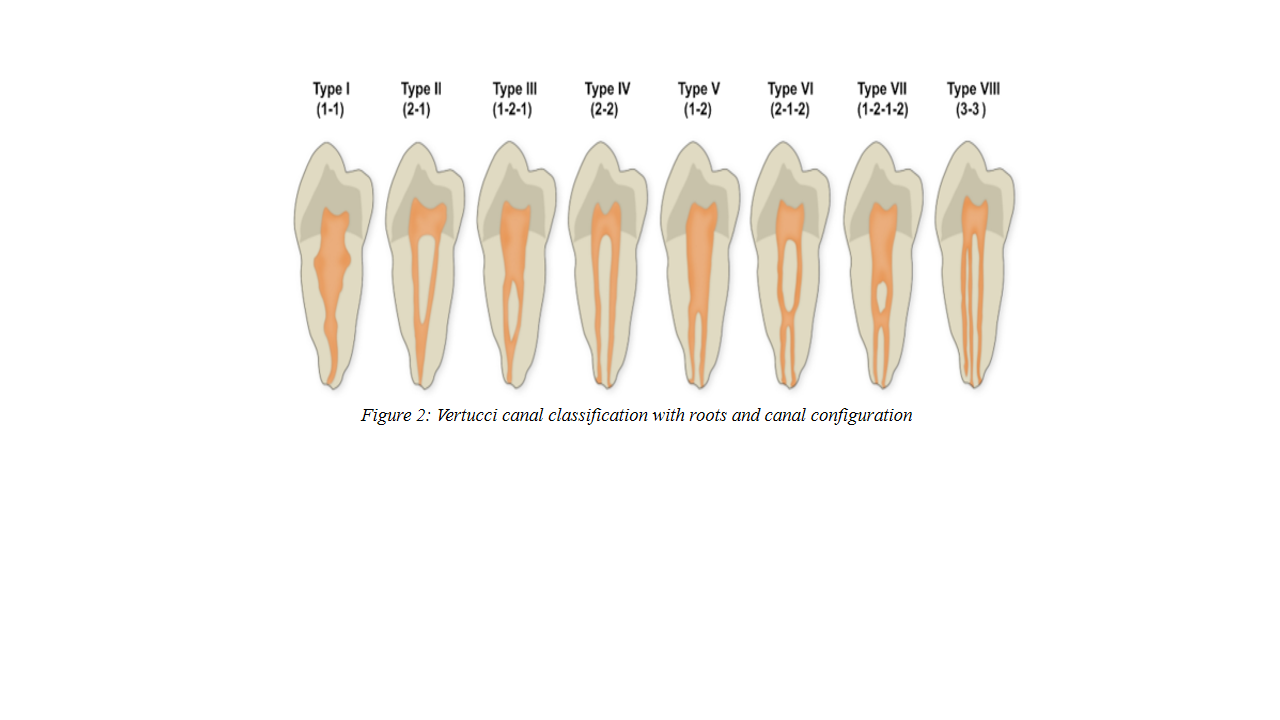
Maxillary first premolars have high variation in internal canal configuration, mesial root concavity, and variation in pulp cavity configuration. Furthermore,increased variation has been reported in several studies which state premolars as the set of teeth which are difficult to treat due to their extreme canal variations.7,8A Chinese study showed that among 1118 Cone-beam computed tomography (CBCT)scans, 94.2% (1053) are single-rooted and 55.1% (616) have one canal in maxillary second premolars.9In another CBCT study on Chilean subpopulation,1070 CBCT scans showed first premolar have one root in 64.86 % of cases and two roots in 35.15 %. Maxillary second premolar presented one root in 66.67 % of cases and two roots in 33.33 %. The frequency of one and two canals was observed to be 30 % and 70 % respectively.Historically, various canal classification systemshave been introduced to study the morphology of permanent teeth, including Weine,11Vertucci,12and Gulabivala’s13classifications. Vertucci classification is commonly adopted and includes eight categories; Type I (1), Type II (2-1), Type III (1-2-1). Type IV (2), Type V (1-2) Type VI (2-1-2), Type VII (1-2-1-2), Type VIII (3).12
Several in vitro and in vivo techniques have been used to analyzethe internal canal structure of human teeth. The most common technique used is Conventional radiography (intraoral radiographs).14 Limitation of this technique includes superimposition of anatomical structures and therefore image distortions, intraoral placement of film, which is sometimes difficult in limited mouth opening, stimulation of gag reflex andusing bisecting angle technique in patients having shallow palatal vaults are among the few.CBCT provides comprehensive and accurate information in three dimensions without the complications associated with techniques and patient factors. Several studies have concluded that CBCT is more accurate in configuring canal architecture than conventional radiography.15
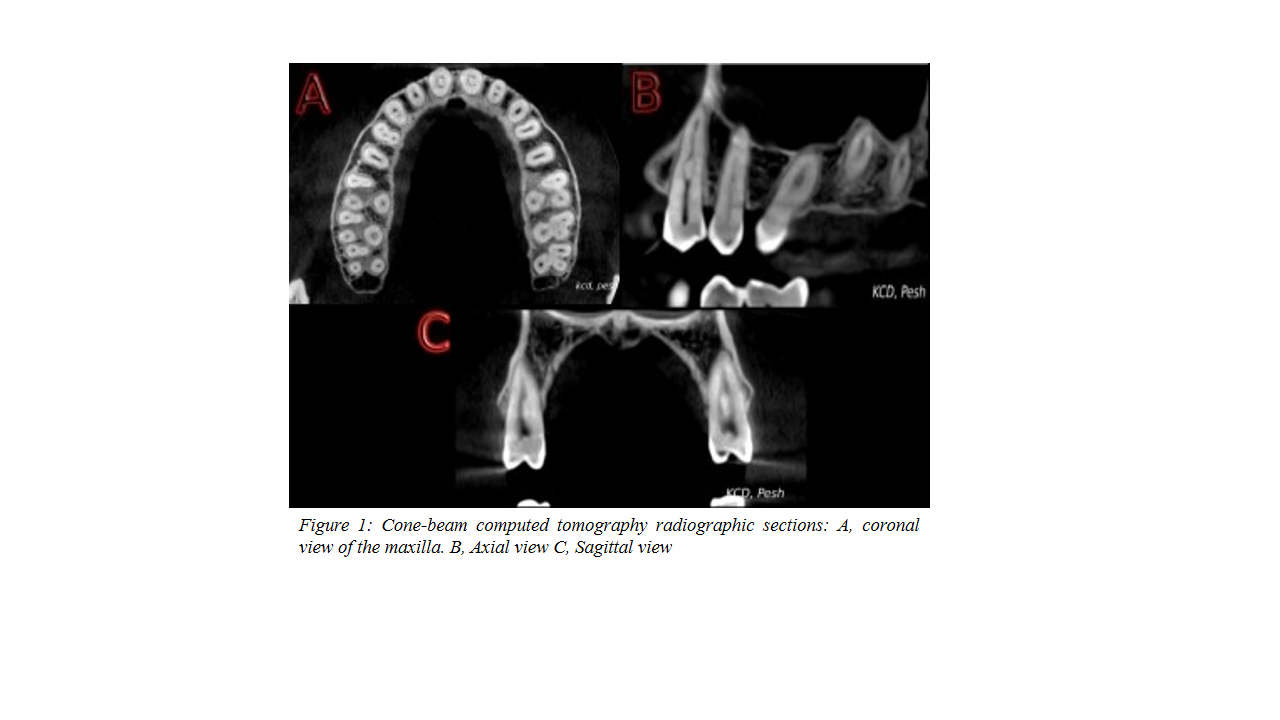
CBCT10,16 is a three-dimensional approach to examine maxillofacial structures (Axial, Sagittal, and Coronal) without structural overlapping and unwanted magnification.(Figure 1A-C). The benefits of the current study included better knowledge of the canal configuration of premolar roots leading to successful clinical outcome. Reducing the treatment failure rate will enhance the quality of life of the patient.
The study's aim was morphology of root canals in maxillary first/second premolars using Vertucci classification and the crown/root lengths of the premolars to compare with other populations using CBCT scans.The rationale of this study was to findout the variations in root canal morphology of maxillary premolars inthe Pakistani north-west region.
METHODS
This study was approved by the ethical committee of the Khyber College of Dentistry (No: 1496-A/ERB/KCD). A sample size calculator ‘Epiinfo software’was used by assuming the prevalence of 15% with a 5% margin of error and 95% confidence level.CBCT images(n =133)of maxillary premolar teeth wereacquired to be evaluated for this cross-sectional study.CBCT scanswere randomlychosen from digital bank of radiology department of Khyber College of Dentistry, Peshawar from July 1st to 30th December,2020.The sampling was purposive with inclusion criteria consisted of at least one premolar in the maxillary arch with fully developed roots and closed apices. Distorted CBCT images, teeth with prosthetic crowns, periapicalpathologies, carious lesions, root canal treated, open apices and apical root resorptions were excluded from the study.
The CBCT unit used was PlanmecaPromax 3D 5.1.0.R (Planmeca Oy, Helsinki, Finland) with an isotropic Voxel size of 70-400 micrometer & a field of view of Ø42x50mm.Radiation Exposures were 90-120kVp and 6.3mA.The CBCT scans were anticipatedby the same company’s viewer Software model 5.1.0.R (Planmeca OY) on hpProfessional Intel(R)graphic control panel workstation (hp Inc) using windows 10 service pack and 40-inch LED monitor with a resolution of 1680-1050 pixels in a low intensity lighted office. Resolution/magnification of the scans was adjusted using windows 10image editing tool to confirmoptimal visualization. Two trained observers wereselected for reading the CBCT images. These observers evaluated the CBCT images using axial, sagittal and coronal views to identify root and root canal morphology and the crown/root lengths of maxillary premolars.The CBCT scans were carefully observed, and the findings were recorded using a proforma with inclusion and exclusion criteria. Inter-examiner variability was analyzed using Cohen kappa test.
During examination, roots& canals count,and configuration of canal system were determined using Vertucci classification in addition to crown/root lengths. Vertucci root canal classification17is adopted and includes eight categories; Type I (1), Type II (2-1), Type III (1-2-1). Type IV (2), Type V (1-2) Type VI (2-1-2), Type VII (1-2-1-2), Type VIII (3) [Figure2].
Patients were classified into 5 age groups: 14-20 years, 21-30 years, 31-40years, 41-50 years, and 51-60 years, with mean 35.3 yrs.and standard deviation of 11.4.Data were analyzed using SPSS (Statistical Package for Social Sciences) version 23. Chi square test with a p value of less than 0.05 was considered significant.
RESULTS
Out of 133 patients, 89 (66.9%) were males and 44 (33.1%) were females. Age wise distribution shows 12 (9%) patients from 14-20 years’ age group, 34 (25.6%) from 21-30 years, 48 (36.1%)were 31-40 years, 24 (18%) were from 41-50 years and 15(11.3%)were from 51-60 years’ age group.
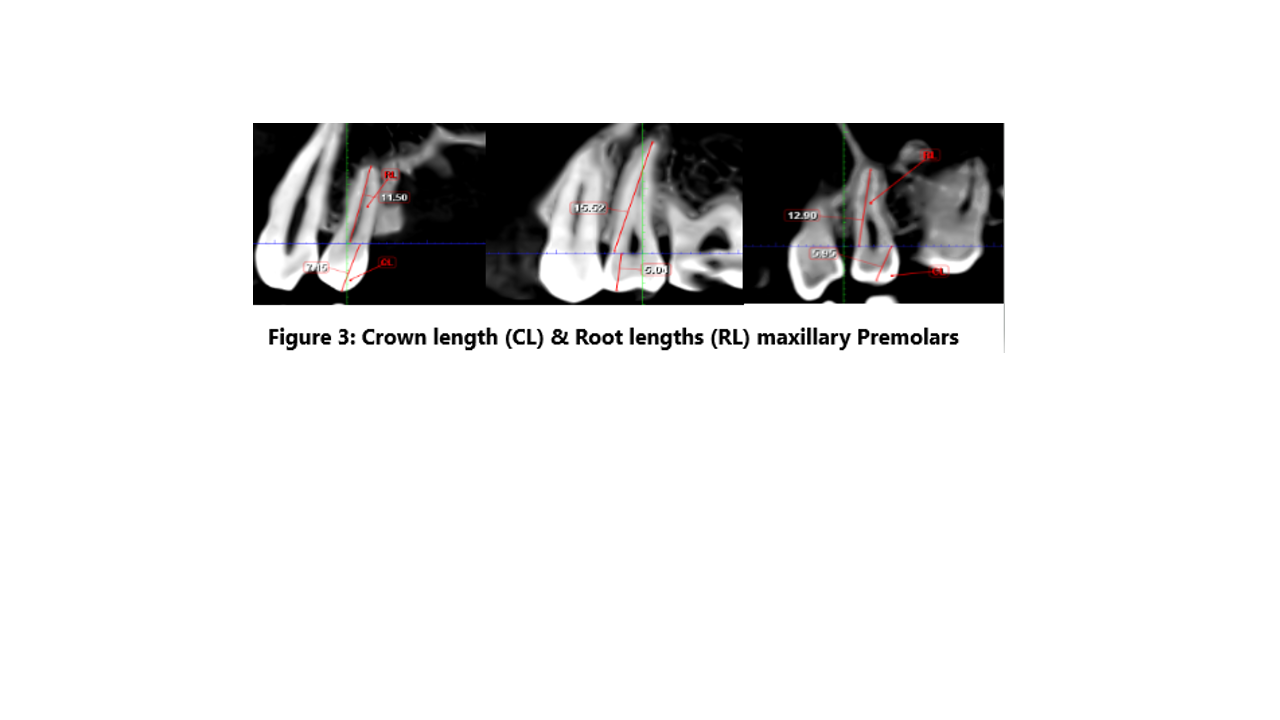
Mean tooth length of maxillary first and second premolar was 19.40±2.035 mm and 20.08±2.395 mm respectively. Mean crown length of maxillary first and second premolar was 6.05±0.752 mm and 5.69±0.505 mm respectively (Figure 3).
Measure of agreement through kappa for number of roots and canal configuration shows 0.92 inter-examiner agreement for maxillary first premolars & 0.88 for maxillary second premolars, respectively. The inter-examiner reliability values show that the method was predictable for evaluation and recording executed by observers. Maximum roots reported for both premolars were three.
In the first premolar teeth, 247 (92.8%) were single-rooted, while 19(7.14%)were two-rooted. In the second premolars, 155(58.27%) were single-rooted, 110(41.35%) were two-rooted and one (0.37%) was three-rooted (Table I).Gender-based distribution revealed that single-root was the commonest root among males (92.7% & 58.4%) and females (30.8% and 19%) among first &second premolar maxillary teeth respectively.
Table I: Root distribution patterns in maxillary premolar teeth by gender
|
Maxillary Premolar Teeth |
Gender |
Number of Roots |
|||
|
One Root |
Two Roots |
Three Roots |
Total |
||
|
First Premolars |
Male |
165 (92.7%) |
13 (7.3%) |
0 |
178 (66.9%) |
|
Female |
82 (93.2%) |
6 (6.8%) |
0 |
88 (33.1%) |
|
|
Total |
247(92.8%) |
19(7.14%) |
0 |
266(100%) |
|
|
Second Premolars |
Male |
104 (58.4%) |
73(41%) |
1 (0.6%) |
178 (66.9%) |
|
Female |
51(58%) |
37(42%) |
0 (0%) |
88 (33.1%) |
|
|
Total |
155(58.27%) |
110 (41.35%) |
1(0.37%) |
266(100%) |
|
Type I canal composition was most common in first premolars (45.4%), followed by Type IV (25.9%), Type V (12%), Type III (10.9%) & Type II (3.4%). Similarly, Type I canal classification was most prevalent in second premolars (64.2%), followed by Type III (15.4%), Type V (8.6%), Type IV (4.5%) & Type II (4.1%) respectively (Table II).
Table II: Canal configuration variability in maxillary premolar teeth by gender and type
|
Maxillary Premolar Teeth |
Gender |
Canal Configuration |
||||||||
|
Type I |
Type II |
Type III |
Type IV |
Type V |
Type VI |
Type VII |
Type VIII |
Total |
||
|
First Premolars
|
Male |
86 (32%) |
8 (3.0%) |
17 (6.3%) |
42 (15.7%) |
20 (7.5%) |
0 |
4 (1.5%) |
1(0.37%) |
178 (100%) |
|
Female |
35 (12%) |
1 (0.3%) |
12 (4.5%) |
27 (10.1%) |
12 (4.5%) |
1 (0.3%) |
0 |
0 |
88 (33.1%) |
|
|
Total |
121 (45.4%) |
9 (3.4%) |
29 (10.9%) |
69 (25.9%) |
32 (12%) |
1 (0.3%) |
4 (1.5%) |
1 (0.3%) |
266 (100%) |
|
|
Second Premolars |
Male |
113 (42.8%) |
6 (2.2%) |
32 (12%) |
6 (2.2%) |
17 (6.3%) |
2 (0.7%) |
2 (0.7%) |
0 |
178 (66.9%) |
|
Female |
58 (21.8%) |
5 (1.8%)
|
9 (3.3%) |
6 (2.2%) |
6 (2.2%) |
0 |
4 (1.5%) |
0 |
88 (33.1%) |
|
|
Total |
171 (64.2%) |
11 (4%) |
41 (15.4%) |
12 (4.5%) |
23 (8.6%) |
2 (0.7%) |
6 (2.2%) |
0 |
266 (100%) |
|
Three rooted teeth (0.37%) were only observed in males and none in females. Comparison of gender difference and canal count in all maxillary
Table III: Root canal configuration analysis of maxillary premolars by teeth position and gender
|
Teeth Position |
Gender |
1 Canal |
2 Canals |
3 Canals |
Chi square |
DF |
P value |
|
Maxillary Left first Premolar |
Male |
13 (4.8%) |
76 (28.5%) |
0 |
1.35 |
1 |
0.17 |
|
Female |
10 (3.7%) |
34 (12.7%) |
0 |
||||
|
Maxillary right first Premolar |
Male |
16 (6.0%) |
72 (27%) |
1 (0.3%) |
0.53 |
2 |
0.73 |
|
Female |
7 (2.6%) |
37 (13.9%) |
0 |
||||
|
Maxillary Left second Premolar |
Male |
47 (17.6%) |
42 (15.8) |
0 |
2.85 |
1 |
0.098 |
|
Female |
30 (11.2%) |
14 (5.2%) |
0 |
||||
|
Maxillary right second Premolar |
Male |
57 (21.4%) |
32 (12.0%) |
0 |
1.61 |
1 |
0.24 |
|
Female |
33 (12.4%) |
11 (4.1%) |
0 |
DISCUSSION
Vertucci et al.,recorded the average length of first premolar to be 20.6mm and Pecora et al.,reported it 21mm.18,19The mean tooth length found in the current study was 19.40mm which is comparable to previous studies. Similarly, tooth length found by Raj et al.,20 forsecond premolar was 21.5mm and by Vertucci as 21.5mm which was comparable to current study findings. The mean crown height for the first premolar was 6.05mm and for the second premolar, 5.69mm.These findings showed that there was no significant difference between the tooth lengths in different study populations. These findings were also comparable to other investigators.21,22
Gender distribution showed that there was no statistically significant difference in number of roots between males and females study population, only a single case of three rooted teeth wasfound in males.No three rooted teeth were reported in the second premolar in both genders. This contrasts with the data reported byCelikten et al.,23 which showedstatistically significant difference (p≤ 0.05) in gender for maxillary first premolars while no significance was observed in second premolars.Several studies have analyzed internal anatomy through CBCT imaging, and it has been observed that maxillary first premolars tend to present two roots, but according to geographical regions the frequency varies between 30.3 % on a Chinese subpopulation to 80 % in a French population. 9,24
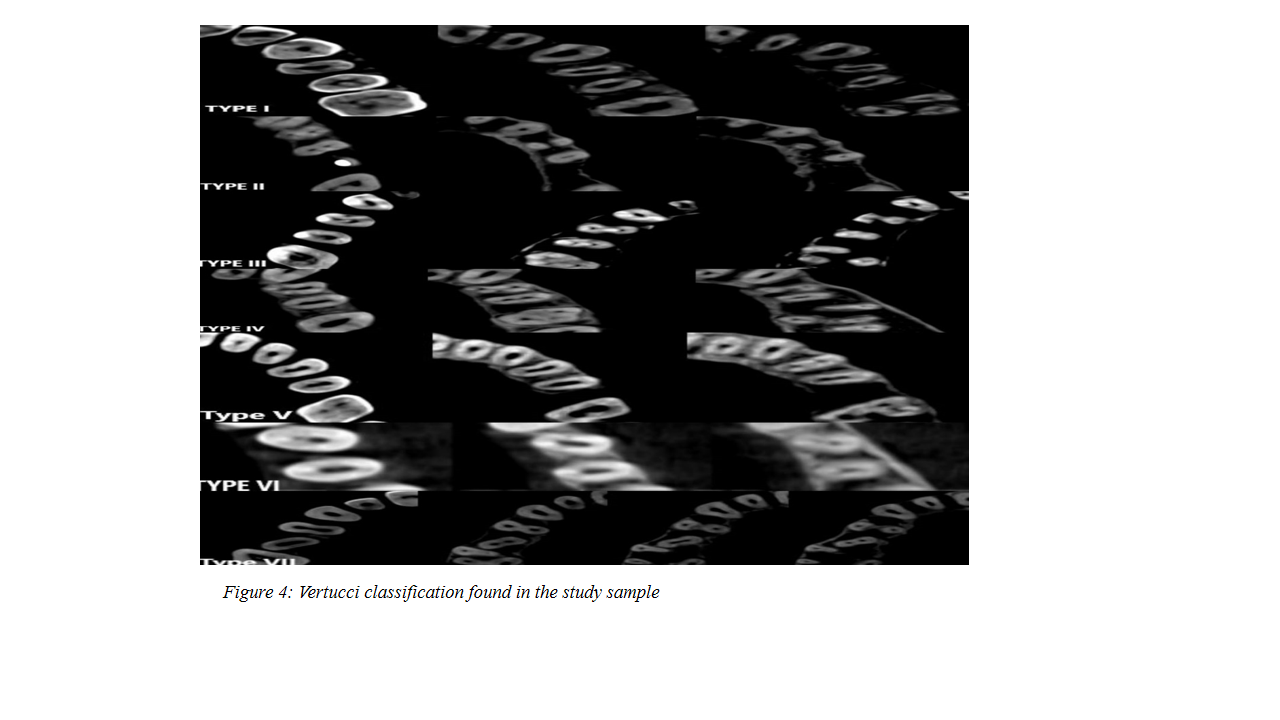
Root count and canal morphology comparison were reported in several studies. According to Bulut et al.,25in first premolars, the Type I (62.6%) was common in Turkish population followed by Type II (34.1%) and Type III (0.8%). These findings were comparable to the present study which reported to have Type I (45.4%), Type IV (25.9%),Type V (12%),Type III (10.9%),Type II (3.4%), Type VII (1.5%) and Type VIII (0.3%) of the cases, in descending order.A study conducted by Alqedairet al.,26showed Type IV (69.1%)to be the most frequent canal composition infirst premolars in Saudi population (Figure 4).
Similarly, in maxillary second premolars,this study showed common canal morphologyrecorded wasType I (64.2%) followed by Type III (15.4%), Type V (8.6%), Type II (4.1%), Type VII (2.2%) and Type VI (0.75%). These results were comparable to the research performed by Bulut et al.,25that showed Type I (77.6%) wereamong the frequent type followed by Type II (12.5%), Type IV (6.6%), Type V (1.9%), Type III (1.3%) and Type VI (0.2%).The current results were also comparable to the study conducted by Alqedair et al.,26 which showed Type I (49.4%) canal configuration to be most common in Saudi population.
One of the major advantages of CBCT is that it is a noninvasive, accurate and prompt method of attaining a three-dimensional image in coronal, axial, and sagittal sections to evaluate the canal morphology with non or minimal overlap of anatomical structures. 27 The maxillary premolars are among the most difficult teeth to treat endodontically due to their variation in number of roots, canal configuration, the direction and longitudinal depressions of the roots, and various pulp cavity configurations. North-west region of Pakistan is unique in a way that many different races were migrated and settled over 100 or more years, inter racial marriages took place and variation in several aspects of human anatomy have occurred, dental variation is part of the human evolution. 28
The current study represented the internal root anatomy of the maxillary first/second premolars in Pakistani population and provided a theoretical basis of clinical care. It is recommended to change the access cavity's orientation from standard oval shape in special situations, depending on the presence of extra canal as defined by CBCT.
The strength of this study was the calculation of inter examiner variability to assess the reliability of the results. Moreover, in addition to canal configuration and number of roots, root length and crown length were also calculated and compared.
The limitation of the study was sample size due to the number of CBCT scans availability and collection of scans from singleinstitution.Furthermore, the spatial resolution of the CBCT in this study was lower than that of micro-CT and Nano CT (Computed Tomography) which may affect the findings. Furthermulticenter studies using more advanced techniques are recommended such as micro-CT to overcome the limitation of this study.
CONCLUSION
Most of the first and second premolars were single rooted.The common canal morphology was Type I in both premolarswhile the other root canal morphology types could be found. Besides that,crown/root lengths were comparable to other study findings. The gender differences for canal count and morphology were not significant.CBCT has proved to be a useful diagnostic tool for in vivo study of dental morphology that increases the success rate of clinical outcomes.
ACKNOWLEDGEMENT
This work was supported by the Radiology department of Khyber College of dentistry, Peshawar, KPK Pakistan. I thank Dr Aamir Mehmood Khan, Assistant Professor in Department of Conservation, Khyber College of Dentistry, for his help in acquisition and interpretation of raw data.
REFERENCES
1. Senan EM, Alhadainy HA, Genaid TM, Madfa AA. Root form and canal morphology of maxillary first premolars of a Yemeni population. BMC Oral Health2018;18(1):94.https://doi.org/10.1186/s12903-018-0555-x
2. Przesmycka A, Jędrychowska-Dańska K, Masłowska A, Witas H, Regulski P, Tomczyk J. Root and root canal diversity in human permanent maxillary first premolars and upper/lower first molars from a 14th–17th and 18th–19th century random population. Arch Oral Biol 2020;110:104603.https://doi.org/10.1016/j.archoralbio.2019.104603
3. Mahmood TR. Management of apical periodontitis using wave one gold reciprocating files, single-cone endodontic approach: A case series. Ann Med Surg (Lond) 2021;66:102385.https://doi.org/10.1016/j.amsu.2021.102385
4. AlmazrouYM, Edrees FA, Alaqeel S, Alqahtani F, Albihlal A. Root canal treatment of maxillary second premolar with two roots and three canals: Two case reports. Saudi EndodJ 2020;10(3):274-8.https://doi.org/10.4103/sej.sej_150_19
5. Maghfuri S, Keylani H, Chohan H, Dakkam S, Atiah A, Mashyakhy M. Evaluation of root canal morphology of maxillary first premolars by cone beam computed tomography in SaudiArabian southern region subpopulation: An in vitro study. Int JDent 2019;2019:1-6.https://doi.org/10.1155/2019/2063943
6. Augusti D, Augusti G. Unexpected complication ten years after initial treatment: Long-term report and fate of a maxillary premolar rehabilitation. Case Rep Dent 2018;2018:3287965. https://doi.org/10.1155/2018/3287965
7. Saber SEDM, Ahmed MHM, Obeid M, Ahmed HMA. Root and canal morphology of maxillary premolar teeth in an Egyptian subpopulation using two classification systems: A cone beam computed tomography study. IntEndod J 2019;52(3):267-278.https://doi.org/10.1111/iej.13016
8. Alnassar FA, Almutairi W, Al-Dahman Y. Radiographic variations of maxillary and mandibular premolars with type V canal configuration – A cone-beam computed tomographic study. Saudi EndodJ2021;11(3):345-9.http://dx.doi.org/10.4103/sej.sej_204_20
9. Yan Y, Li J, Zhu H, Liu J, Ren J, Zou L. CBCT evaluation of root canal morphology and anatomical relationship of root of maxillary second premolar to maxillary sinus in a western Chinese population. BMC Oral Health 2021;21(1):358. https://doi.org/10.1186/s12903-021-01714-w
10. Matus D, Fuentes R, Navarro P, Betancourt P. Morphological analysis of maxillary first premolars by cone beam computed tomography in a Chilean sub-population. Int J Morph 2020;38(5):1266-70.
11. Eskoz N, Weine FS. Canal configuration of the mesiobuccal root of the maxillary second molar. J Endod 1995;21(1):38-42.https://doi.org/10.1016/s0099-2399(06)80555-8
12. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral SurgOral Med Oral Pathol 1984;58(5):589-99.https://doi.org/10.1016/0030-4220(84)90085-9
13. Gulabivala K, Aung TH, Alavi A, Ng YL. Root, and canal morphology of Burmese mandibular molars. IntEndod J 2001;34(5):359-70.https://doi.org/10.1046/j.1365-2591.2001.00399.x
14. Aps JKM, Lim LZ, Tong HJ, Kalia B, Chou AM. Diagnostic efficacy of and indications for intraoral radiographs in pediatric dentistry: A systematic review. EurArch PaediatrDent 2020;21(4):429-62.https://doi.org/10.1007/s40368-020-00532-y
15. Borghesi A, Michelini S, Zigliani A, Tonni I, Maroldi R. Three-rooted maxillary first premolars incidentally detected on cone beam CT: An in vivo study. SurgRadiolAnat 2019;41(4):461-8.https://doi.org/10.1007/s00276-019-02198-8
16. Olczak K, Pawlicka H, Szymański W. Root form and canal anatomy of maxillary first premolars: A cone-beam computed tomography study. Odontology 2021;110(2):365-75. https://doi.org/10.1007/s10266-021-00670-9
17. ShahzadAS. Endodontic management of mandibular second premolar with vertucci root canal configuration type V. Case RepDent 2022;2022:3197393.https://doi.org/10.1155/2022/3197393
18. Vertucci FJ, Gegauff A. Root canal morphology of the maxillary first premolar.J Am Dent Assoc 1979;99(2):194-8.https://doi.org/10.14219/jada.archive.1979.0255
19. Pécora JD, Saquy PC, Neto MDS, Woelfel JB. Root form and canal anatomy of maxillary first premolars. Braz Dent J 1992;2(2):87-94.
20. Raj UJ, Mylswamy S. Root canal morphology of maxillary second premolars in an Indian population. J Conserv Dent 2010;13:148-51.
21. Wang J, Rousso C, Christensen BI, Li P, Kau CH, MacDoughall M, et al. Ethnic differences in the root to crown ratios of the permanent dentition. OrthodCraniofac Res 2019;22(2):99-104.https://doi.org/10.1111/ocr.12288
22. Shahid F, Alam MK, Khamis MF. Maxillary and mandibular anterior crown width/height ratio and its relation to various arch perimeters, arch length, and arch width groups. Eur J Dent 2015;9(4):490-9.https://doi.org/10.4103/1305-7456.172620
23. Celikten B, Orhan K, Aksoy U, Tufenkci P, Kalender A, Basmaci F, et al. Cone-beam CT evaluation of root canal morphology of maxillary and mandibular premolars in a turkishcypriot population. BDJ Open 2016;2(1):15006.https://doi.org/10.1038/bdjopen.2015.6
24. Monsarrat P, Arcaute B, Ove AP, Maury E, Telmon M, Georgelin-Gurgel M, et al. Interrelationships in the variability of root canal anatomy among the permanent teeth: A full-mouth approach by cone-beam CT. PLoS One 2016;11(10):e0165329. https://doi.org/10.1371/journal.pone.0165329
25. Bulut DG, Kose E, Ozcan G, Sekerci AE, Canger EM, Sisman Y. Evaluation of root morphology and root canal configuration of premolars in the Turkish individuals using cone beam computed tomography. EuroJDent 2015;9(4):551-7.https://doi.org/10.4103/1305-7456.172624
26. Alqedairi A, Alfawaz H, Al-Dahman Y, Alnassar F, Al-Jebaly A, Alsubait S. Cone-beam computed tomographic evaluation of root canal morphology of maxillary premolars in a Saudi population. Biomed Res Int 2018;2018:8170620.https://doi.org/10.1155/2018/8170620
27. Ahmed HMA, MusalePK, El Shahawy OI, DummerPMH. Application of a new system for classifying tooth, root and canal morphology in the primary dentition. IntEndod J 2020;53(1):27-35.https://doi.org/10.1111/iej.13199
28. Sadaf A, Huma Z, Javed S, Masood A. Maxillary premolar teeth: Root and canal stereoscopy. Khyber Med Univ J 2019;11(4):240-7. https://doi.org/10.35845/kmuj.2019.19337
|
Following author have made substantial contributions to the manuscript as under:
SAS: Concept and study design, acquisition, analysis and interpretation of data, drafting the manuscript, critical review, approval of the final version to be published
Author agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST Author declared no conflict of interest
GRANT SUPPORT AND FINANCIAL DISCLOSURE Author declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |