![]() https://doi.org/10.35845/kmuj.2023.23029 ORIGINAL ARTICLE
https://doi.org/10.35845/kmuj.2023.23029 ORIGINAL ARTICLE
Impact of optimism on post-traumatic growth of burn survivors: role of emotional intelligence, gender and severity of burn injury
Hina
Sultan 1,3 ![]() ,
Umaira Abid 1, Amna Khawar 2,
Muhammad Ali 3
,
Umaira Abid 1, Amna Khawar 2,
Muhammad Ali 3
|
1: Department of Psychology, Lahore Leads University, Lahore, Pakistan 2: Department of Applied Psychology, Lahore College for Women University, Lahore, Pakistan 3: Department of Applied Psychology, University of the Punjab, Lahore Pakistan
Email Contact #: +92-335-4185624 Date Submitted: September 23, 2022 Date Revised: December 16, 2022 Date Accepted: January 04, 2023 |
|
THIS ARTICLE MAY BE CITED AS: Sultan H, Abid U, Khawar A, Ali M. Impact of optimism on post-traumatic growth of burn survivors: role of emotional intelligence, gender and severity of burn injury. Khyber Med Univ J 2023;15(1):38-43. https://doi.org/10.35845/kmuj.2023.23029 |
ABSTRACT
OBJECTIVES: To examine the mediating role of emotional intelligence (EI) between optimism and post-traumatic growth (PTG) among burn survivors and to see the interaction effects of gender and nature of injury on optimism, emotional intelligence and PTG.
METHODS: This descriptive correlational study was conducted from 2nd January-30th April 2022, at in-patient department of burn centers of three public hospitals of Lahore, Pakistan. Out of 250 survivors of moderate and severe burns, selected through purposive sampling strategy, 229 completed the survey via face to face or call contacts. Participants filled out three structured questionnaires along consent form. Later, collected data was analyzed through PROCESS macro v3.5 and SPSS V23.0.
RESULTS: Out of 229 patients 139 (60.7%) were males and 90 (39.3%) were females. Mean age was 32.4±3.1 years. Optimism had a direct effect on emotional intelligence, emotions perception, emotions utilization, managing self-relevant emotions, managing other’s emotions, and PTG, p<.0001. EI and all its subscales predicted PTG, the overall model explained 36% of variance in dependent variable, significant at R=.60, F (3,226) =151.30, p<.0001. Indirect effects of EI and subscales were found between optimism and PTG. Further, interaction effects of gender and nature of injury were seen for optimism, EI and PTG.
CONCLUSION: Optimistic approaches and stimulating emotional expressions, managing self-relevant emotions, and utilization of positive emotions might help burn survivors in adapting to their trauma in the longer term. Further, both men and women reported post traumatic growth but severity of injury was affecting PTG in men and women equally.
KEYWORDS: Burns (MeSH); Burn survivors (Non-MeSH); Optimism (MeSH); Emotional Intelligence (MeSH); Posttraumatic Growth, Psychological (MeSH); Burns, Inhalation (MeSH); Burns, Chemical (MeSH); Burn Units (MeSH).
INTRODUCTION
Burn wounds are one of the under-appreciated traumas that can affect anybody, anywhere and anytime. The vital reasons behind burn injuries can be hot liquids, a flame or hot grease, fire, electric/chemical sources which can cause mild scars (limited to epidermis only; first degree), moderate (shallow partial-thickness; second degree), to severe deep tissue destruction (third and fourth degree; required surgery).1 Burn injuries are the most severe stressful incidents that can significantly affect the mental health of patients. Statistics indicate that 30- 40% of patients continue to experience long lasting psychological problems following burn trauma. However, patients with different personality traits can perceive the trauma differently as with the gradual popularity of biopsychosocial models, the concentration on patient well-being and post-traumatic growth has become an important matter of concern for researchers.2
The present study presents its primary investigation on the post-traumatic growth of burn individuals, with a focus on two variables; optimism and emotional intelligence. Optimism means patients’ positive expectations for the future regarding trauma recovery.3 Researchers in North Carolina and China found a positive association of optimism with positive emotions, self-esteem, life satisfaction, and subjective well-being among burn survivors.4,5 Further, emotional intelligence refers to understand one’s and others’ emotions and to maintain a control over emotions under unusual circumstances.6 In 2020, Pakistani study showed that dispositional optimism, resilience and emotion coping was related to quality of life among those burned from acid, flame, or hot water.7 In Qatar, a qualitative study elaborated the psychological sufferings of burn survivors however, patients reported that when they started managing their emotions, it resulted in personal growth and appreciation of life.8
However, in Pakistan and in other countries, mostly researchers studied depression, anxiety and other negative emotions among burn survivors.9,10 Especially the above-mentioned literature did not directly focus on optimism with post-traumatic growth (PTG) but so far with other positive psychological states. However, a quantitative study, carried out in UK, directly addressed PTG in burn survivors with coping, perceived support, optimism, etc.11 which also raised our confidence to examine PTG with optimism and especially taking emotional intelligence as a mediator between these variables. So, the current study holds significance to fill out the gap in literature by looking at growth after burn injuries in Pakistani population. Especially, emotional intelligence highlighted the importance of how emotional expression, engagement, and utilization can be a milestone in adaptation and improvement in complications as burned victims have poor facial appearance, suffer from intense pain, and find difficulties in maintaining daily activities. So, instead of thinking about negativity, if survivors focus on PTG, they can recognize new possibilities in life, strengthen relationships with others, and can grow positively. Also, at clinical level, we describe some specific means by which a therapist can create an atmosphere for growth for burn survivors. Moreover, researches specify that adult men and women have different etiology of behind burning and men are more prone to burn related injuries but studies suggest no gender differences in seeking medical care based on the severity of injury but a few suggest that women are given extra attention while a few negate these findings.12 Thus, the present study aimed to examine the mediating role of emotional intelligence between optimism and post-traumatic growth among burn survivors and to see the interaction effects of gender and nature of injury on optimism, emotional intelligence and post-traumatic growth.
METHODS
This descriptive correlation study was approved by ethical review committee of University of Lahore, Pakistan (reference number# ERC/27-12-21/351). For this study, data was collected from in-patient department of burn centers of three public hospitals of Lahore, Pakistan from 2nd January-30th April 2022. At first, informed consent was taken from patients or patients’ family members. Adopting convenient sampling strategy, sample size was calculated by G power,13 with α error =.05, and for five predictors, an estimated sample size was 200-250, thus 250 patients were taken and during the entire month of January, basic information regarding patients' gender, age, nature of burn injury, etc. was taken from hospital staff. After an interval of 3 months, patients were contacted again via phone calls to collect data (during April 2022, as three months’ gap is usually considered enough to evaluate PTG in trauma survivors). After 3 months, 10 patients refused to be the part of study while 11 questionnaires were discarded due to incomplete information. Finally, 94 patients responded on call while 135 completed the questionnaires face to face during follow up with their doctors in April. Thus, 229 patients of both genders, ranging in age from 20-50 years, married or unmarried, answered the survey that included moderate and severely injured patients, burned through stove/pressure cooker/gas cylinder blast, boiled water, set fire on clothes, through vehicle accidents or while working in automobiles repairing shops. Doctors determined moderate and severe burn injury by applying the rules of nine. For instance, the front and back of the head and neck equals 9% of the body area. So, patients scoring 20-25% were considered as moderate while those with at least 26-30% were considered as severely burnt out.14Completely disabled, amnesiacs, and above 50 years’ patients were excluded because they had multiple comorbidities, which could bias the data. Participants filled out Demographic Information, Life Orientation Test Revised (1994) which is a standard psychological instrument, comprised of 10 items, that assesses one’s dispositional level of optimism with score format strongly disagree (0) to strongly agree (4). In the current study, reliability of Urdu version of this scale was significant α=.69.15 Emotional Intelligence Scale developed by Schutte in 1998 and later validated many times at different general and clinical patients. It consists of 33 items with score format 1 (strongly disagree) to 5 (strongly agree).16 For present study, it was translated in Urdu and alpha reliability of translated version was α=.88. Urdu translated version of Post-Traumatic Growth Inventory-Short Form, consisted of 10 items was also filled out. This is a six-point Likert scale with score format 0-5.17 Participants did not find out any ambiguity in understanding the items. The participation time was 30-45 minutes. In the end, researchers thanked the participants for their cooperation and analyzed the data via PROCESS macro v3.5 for mediation analysis and SPSS V23 for descriptive statistics and MANOVA.
RESULTS
Out of 229 patients 139 (60.7%) were males and 90 (39.3%) were females, ranging in age from 20-50 years and mean age was 32.4±3.1 years.
Out of 229 survivors, 87 (37.99%) were married while 142 (62%) were unmarried. There were different reasons behind burning mentioned in the table I and the nature of injury among survivors was either moderate (n=123; 53.71%) or severe (n=106; 46.28%). Patients had injuries on different body parts like few had injuries on head and neck while some had wounds on arms, buttocks, or chest, varied from individual to individual (see Table I).
Table I: DEMOGRAPHIC PROFILE OF BURN PATIENTS
|
Variables |
Frequency (n=229) |
Percentage |
|
|
Gender |
Males |
139 |
60.69 |
|
Females |
90 |
39.30 |
|
|
Age (years) |
20-30 |
99 |
43.23 |
|
>30-40 |
78 |
34.06 |
|
|
>40-50 |
52 |
22.70 |
|
|
Marital Status |
Married |
87 |
37.99 |
|
Unmarried |
142 |
62 |
|
|
Reasons of Assault |
Boiled water |
11 |
4.80 |
|
Stove blast |
5 |
2.18 |
|
|
Burnt by vehicle accidents |
123 |
53.71 |
|
|
Cylinder blast |
7 |
3.05 |
|
|
Pressure Cooker blast |
9 |
3.93 |
|
|
Burnt out while working in automobile shops/ welding/mechanical work |
52 |
22.70 |
|
|
Set fire on clothes |
22 |
9.60 |
|
|
Nature of injury |
Moderately burnt (head/neck/back/chest/arms/abdomen/Buttocks) |
123 |
53.71 |
|
Severely burnt (abdomen/head/neck/chest/back/arms/buttocks) |
106 |
46.28 |
|
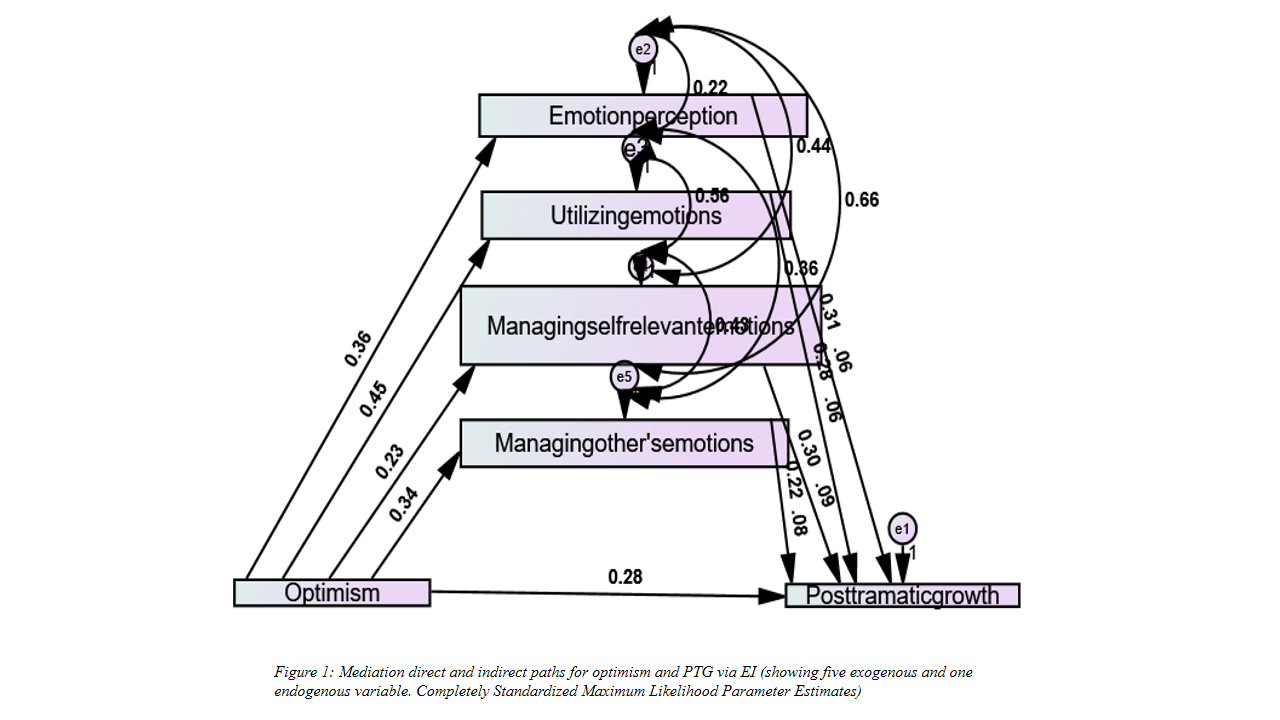
Table II revealed that optimism had a direct effect on EI (β=.56, p<.0001); Emotions Perception (EP) [β=.34, p<.0001]; Utilization of Emotions (UE) [β=.23, p<.001]; Managing self-relevant emotions (MSRE) [β=.45, p<.0001]; and Managing other’s emotions (MOE) [β=.36, p<.0001]; the overall model explained 42% of variance, R=.65, F (3,226) =94.89, p<.0001. All subscales of EI were significantly associated with each other, p<.0001. Outcomes indicated that optimism had a direct effect on PTG (β=.28, p<.0001); EI (β= .57, p<.0001) and it’s all subscales, EP (β=.31, p<.0001); UE (β=.28, p<.001); MSRE (β=.30, p<.0001); and MOE (β=.22, p<.001) were predicting PTG, the overall model explained 36% of variance in dependent variable, significant at R=.60, F (3,226) =151.30, p<.0001.
Table II: STANDARDIZED ESTIMATES OF DIRECT EFFECTS OF OPTIMISM AND EI (SUBSCALES) ON PTG
|
Variables |
Optimism |
EI |
EP |
UE |
MSRE |
MOE |
PTG |
|||||||
|
Β |
SE |
|
|
β |
SE |
β |
SE |
β |
SE |
β |
SE |
β |
SE |
|
|
Optimism |
1 |
.00 |
.56 |
|
.34 |
.03 |
.23 |
.04 |
.45 |
.09 |
.36 |
.03 |
.28 |
.01 |
|
EI |
.56 |
.01 |
1 |
|
.44 |
.01 |
.34 |
.02 |
.47 |
.02 |
.51 |
.01 |
.57 |
.03 |
|
EP |
.34 |
.03 |
.44 |
|
1 |
.00 |
.22 |
.05 |
.44 |
.05 |
.66 |
.06 |
.31 |
.04 |
|
UE |
.23 |
.04 |
.34 |
|
.22 |
.05 |
1 |
.00 |
.56 |
.04 |
.36 |
.05 |
.28 |
.05 |
|
MSRE |
.45 |
.09 |
.47 |
|
.44 |
.05 |
.56 |
.04 |
1 |
.00 |
.43 |
.02 |
.30 |
.00 |
|
MOE |
.36 |
.03 |
.51 |
|
.66 |
.06 |
.36 |
.05 |
.43 |
.02 |
1 |
.00 |
.22 |
.03 |
|
R |
.65*** |
|
.70*** |
|
.55*** |
|
.50*** |
|
.52*** |
|
.75*** |
|
.60*** |
|
|
R2 |
.42*** |
|
.49*** |
|
.30*** |
|
.25*** |
|
.27*** |
|
.56*** |
|
.36*** |
|
|
F |
94.89 |
|
134.56 |
|
26.78 |
|
121.90 |
|
34.26 |
|
161.30 |
|
151.30 |
|
Note. EP=Emotions Perception; UE=Utilization of Emotions; MSRE= Managing self-relevant emotions; MOE: Managing other’s emotions; PTG = Post-Traumatic Growth; β=standardized regression coefficient; SE=Standard Error; **p<.001; ***p<.0001
Table III depicted that EI had an indirect effect between optimism and PTG, β=.09, p<.0001. Also, EP, β=.08, p<.0001; UE, β=.09, p<.0001; MSRE, β=.06, p<.0001; and MOE, β=.06, p<.0001 established relationships between optimism and PTG. So, EI had a buffer effect on PTG of burn survivors.
Table III: STANDARDIZED ESTIMATES OF INDIRECT EFFECTS VIA EI BETWEEN OPTIMISM AND PTG
|
Variables |
EI-PTG |
EP-PTG |
UE-PTG |
MSRE-PTG |
MOE-PTG |
|||||
|
β |
SE |
SE |
β |
SE |
β |
SE |
β |
SE |
||
|
Optimism |
.09*** |
.03 |
.08*** |
.04 |
.09*** |
.05 |
.06*** |
.04 |
.06*** |
.04 |
Note. EP=Emotions Perception; UE=Utilization of Emotions; MSRE= Managing self-relevant emotions; MOE: Managing other’s emotions; PTG= Post-Traumatic Growth; β=standardized regression coefficient; SE=Standard Error***p<.0001
Multivariate analysis of variance showed that men and women burned patients did not differ in manifesting optimism, EI, and PTG, p>.05 (Table IV). However, it was revealed that moderately burnt patients (M=24.12, SD=.03) were more optimistic than severely burnt (Mean=20.78, SD=1.34), t(226)= -4.56, p=.00. Results manifested that moderately burnt patients were more emotionally intelligent than severely burnt, t (226) = -6.89, p=.00. Similar findings were also reported for PTG by burn survivors but we found an interaction effect of gender and nature of injury. Further analysis revealed that both men and women with severe burn injuries were less optimistic, emotionally intelligent and reported less growth after trauma.
Table IV: MANOVA FOR GENDER AND NATURE OF INJURY
Note. EI=Emotional Intelligence; PTG=Post Traumatic Growth; F=ANOVA; *p<.05; SD: Standard deviation
Figure 1 also displayed the direct effects of optimism and EI subscales on PTG which were significant p<.001. It also depicted that EI subscales mediated the relationship between optimism and PTG significant at p<.001.
DISCUSSION
It is usually evident that any kind of traumatic event like floods, earthquakes, accidents or burns impact the psychological health of victims badly. However, nature has made the humans so flexible and courageous that they can come out of adversity and move towards a normal life.18 In the present study, it was also seen that burn survivors had an optimistic personality and this optimism had significant association with EI, and all its components; EP, UE, MSRE, and MOE. An optimistic approach specified that though circumstances were not good enough but survivors were hopeful for the better things coming into their way in future. Although researches have shown that extreme physical pain caused by wound dressings, transplantation, and other treatments, patients experience physical after effects such as changes in skin color, itching, contractures, and impaired mobility, along psychological problems such as feelings of loss, depression, anger, and anxiety throughout and following the burn treatment process.19,20 However, a study in China found that burn survivors gain a new understanding of life.21 Another study on over 16 years of burn survivors used optimistic approach to combat with trauma which found to be linked with emotional stability.22
Results also showed the survivors’ capabilities to appraise their emotions positively, and regulate emotions in the self and others. A positive emotional functioning inserted direct effects on optimism and PTG and also established an indirect effect between theses constructs. PTG reflected into personal strength and positive apperception of life. A recent study carried out in Korea also showed that social support and positive approach was associated with PTG in mild, moderate and severe burn srvivors.23 In another study, results showed that depression, anxiety, and negative emotions were deteriorating PTG among burn survivors so, positive emotions are mandatory for growth.24 Though, direct studies on burn survivors were not found out but in Asia, UK and America researchers found that optimism and EI are one of the most commonly studied intrapersonal coping resources for anticipating PTG among patients suffering from multiple kinds of diseases thus indirectly supporting our findings as well.25-27
Further, it was interesting to find out that no gender differences were seen in optimism, EI, and PTG while Asian and European studies suggest that men show more PTG after trauma as women are more affected emotionally underwent any type of trauma like earth quake, burns, or floods.28-30 However, our further inquiry helped in reducing these different results as it was seen that basically both men and women were equally affected by the severity of injury and were less optimistic, less emotionally intelligent and less grew than those who were moderately injured.
LIMITATIONS AND SUGGESTIONS
The current study carries some limitations as PTG was not measured among burn survivors in different age groups, literate or illiterate, belonging to different social backgrounds and among those who were married or unmarried. So, in future, these variables should be taken into consideration. There were also methodological flaws like no cause-and-effect relationship could be established due to correlational nature of study. Also, a longitudinal study was needed to carry out because burn injuries, even healed out, but leave a long-lasting impact on a person’s appearance, so, it is necessary to examine how long a survivor can show PTG in further studies. Though, data is generalizable within Lahore city but results cannot be applicable across other cities and regions of Pakistan. thus, it is suggested to collect data from different cities of Pakistan.
CONCLUSION
REFERENCES
1. Jeschke MG, van Baar ME, Choudhry MA, Chung KK, Gibran NS, Logsetty S. Burn injury. Nat Rev Dis Primers 2020;6(1):11. https://doi.org/10.1038/s41572-020-0145-5
2. Enns J, Gawaziuk JP, Khan S, Chateau D, Bolton JM, Sareen J, et al. Mental and physical health outcomes in parents of children with burn injuries as compared with matched controls. J Burn Care Res 2016;37(1):e18-26. https://doi.org/10.1097/bcr.0000000000000309
3. Carlos L, Querido A. Hope and optimism as an opportunity to improve the “Positive Mental Health” demand. Front Psychol 2022;13:827320. https://doi.org/10.3389/fpsyg.2022.827320
4. Foster KN, Holmes JH. Inhalation injury: State of the science. J Burn Care Res 2017;38(3):137-41. https://doi.org/10.1097/bcr.0000000000000539
5. Karimi L, Leggat SG, Bartram T, Afshari L, Sarkeshik S, Verulava T. Emotional intelligence: predictor of employees’ wellbeing, quality of patient care, and psychological empowerment. BMC Psychol 2021;9(1):93. https://doi.org/10.1186/s40359-021-00593-8
6. He F, Cao R, Feng Z, Guan H, Peng J. The impacts of dispositional optimism and psychological resilience on the subjective well-being of burn patients: A structural equation modelling analysis. PLoS One 2013;8(12):e82939. https://doi.org/10.1371/journal.pone.0082939
7. Batool I, Malik G, Fatima S, Manzoor I. Investigation of dispositional optimism, psychological resilience, coping strategies and quality of life among burn survivors. Khyber Med Univ J 2020;12(4):310-14. https://doi.org/10.35845/kmuj.2020.19794
8. Garcia MJS, Kunjavara J. Experiences and Perspectives of the Burn Survivors: Inputs for Protocol Development. J Nurs Pract 2021;4(2):327-33. https://doi.org/10.36959/545/401
9. Yarney L, Yeboah E, Hansen-Garshong R. Experiences of burn patients in Ghana: A qualitative study at the Korle-Bu teaching hospital in Accra. Indian J Burns 2019;27(1):49-56. https://doi.org/10.4103/ijb.ijb_18_19
10. Jain M, Khadilkar N, De Sousa A. Burn-related factors affecting anxiety, depression and self-esteem in burn patients: an exploratory study. Ann Burns Fire Disasters 2017;30(1):30-4.
11. Baillie SE, Sellwood W, Wisely JA. Post-traumatic growth in adults following a burn. Burns 2014;40(6):1089-96.. https://doi.org/10.1016/j.burns.2014.04.007
12. Blom L, Klingberg A, Laflamme L, Wallis L, Hasselberg M. Gender differences in burns: A study from emergency centres in the Western Cape, South Africa. Burns 2016;42(7):1600-8. https://doi.org/10.1016/j.burns.2016.05.003
13. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav Res Methods 2009;41(4):1149-60. https://doi.org/10.3758/brm.41.4.1149
14. Thom D. Appraising current methods for preclinical calculation of burn size - A pre-hospital perspective. Burns 2017;43(1):127-36. https://doi.org/10.1016/j.burns.2016.07.003
15. Waseem R, Ahsan S, Akhter A. Life orientation test- revised: Translation and validation in Pakistan. Multicult Educ 2021;7(11):137-40. https://doi.org/10.5281/zenodo.5669331
16. Schutte NS‚ Malouff JM‚ Simunek M‚ McKenley J, Hollander S. Characteristics of emotional intelligence and emotional wellbeing. Cogn Emot 2002;16(6):769-85. https://doi.org/10.1080/02699930143000482
17. Aslam N, Kamal A. Assessing positive changes among flood affected individuals: translation and validation of Posttraumatic Growth Inventory-Short Form. Pak J Medical Res 2019;58:59-65.
18. Martin L, Rea S, Wood F. A quantitative analysis of the relationship between posttraumatic growth, depression and coping styles after burn. Burns 2021;47(8):1748-55. https://doi.org/10.1016/j.burns.2021.05.019
19. Van Loey NE, Klein-Konig I, de Jong AEE, Hofland HWC, Vandermeulen E, Engelhard IM. Catastrophizing, pain and traumatic stress symptoms following burns: A prospective study. Eur J Pain 2018;22(6):1151-59. https://doi.org/10.1002/ejp.1203
20. Van Loey NEE, de Jong AEE, Hofland HWC, van Laarhoven AIM. Role of burn severity and posttraumatic stress symptoms in the co-occurrence of itch and neuropathic pain after burns: A longitudinal study. Front Med (Lausanne) 2022;9:997183. https://doi.org/10.3389/fmed.2022.997183
21. Li N, Cheng H, Lv L. The relationship between posttraumatic growth, self-efficacy, and social support in burn patients: A cross-sectional study. Burns 2022;48(7):1626-31. https://doi.org/10.1016/j.burns.2022.08.009
22. Lodha P, Shah B, Karia S, De Sousa A. Post-Traumatic Stress Disorder (PTSD) Following Burn Injuries: A Comprehensive Clinical Review. Ann Burns Fire Disasters 2020;33(4):276-87.
23. Hwang S, Lim EJ. Factors associated with posttraumatic growth in patients with severe burns by treatment phase. Nurs Open 2020;7(6):1920-27.
24. Martin L, Byrnes M, Bulsara MK, McGarry S, Rea S, Wood F. Quality of life and posttraumatic growth after adult burn: A prospective, longitudinal study. Burns 2017;43(7):1400-10. https://doi.org/10.1016/j.burns.2017.06.004
25. Kunz S, Joseph S, Geyh S, Peter C. Coping and posttraumatic growth: A longitudinal comparison of two alternative views. Rehabil Psychol 2018;63(2):240-9. https://doi.org/10.1037/rep0000205
26. Kunz S, Joseph S, Geyh S, Peter C. Perceived posttraumatic growth and depreciation after spinal cord injury: Actual or illusory? Health Psychol 2019;38(1):53-62. https://doi.org/10.1037/hea0000676
27. Wong, C.C.Y., Yeung, N.C.Y. Self-compassion and Posttraumatic growth: Cognitive processes as mediators. Mindfulness 2017;8:1078-87. https://doi.org/10.1007/s12671-017-0683-4
28. Lodhi SZ, Gul S, Khattak A. A Qualitative Study on Posttraumatic Growth Processes in Trauma Victims: Evidence from Pakistan. Pshychiatr Danub 2022;34(2):263-72.
29. Barlow MR, Hetzel-Riggin MD. Predicting posttraumatic growth in survivors of interpersonal trauma: Gender role adherence is more important than gender. Psychol Men Masc 2018;19(3):446-56. https://doi.org/10.1037/men0000128
30. Asim M, Van Teijlingen E, Sathian B. Coronavirus Disease (COVID-19) and the risk of Post-Traumatic Stress Disorder: A mental health concern in Nepal. Nepal J Epidemiol 2020;10(2):841-4. https://doi.org/10.3126/nje.v10i2.29761
|
Following authors have made substantial contributions to the manuscript as under:
HS: Concept and study design, acquisition, analysis and interpretation of data, drafting the manuscript, approval of the final version to be published. UA & AK: Analysis and interpretation, drafting the manuscript, approval of the final version to be published. MA: Acquisition of data, critical review, approval of the final version to be published.
Authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST Authors declared no conflict of interest
GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |