![]() https://doi.org/10.35845/kmuj.2023.22823 ORIGINAL ARTICLE
https://doi.org/10.35845/kmuj.2023.22823 ORIGINAL ARTICLE
Serum E-Cadherin level in various clinical variants of oral potentially pre-malignant disorders
Abdus Saboor 1,2, Muhammad Mumtaz Khan 1,
Badsha Afsar 2 ![]() ,
Abbas Saleem Khan 1
,
Abbas Saleem Khan 1
|
1: Department of Pathology, Peshawar Dental College, Peshawar, Pakistan 2: Saidu College of Dentistry, Swat, Pakistan Email Contact #: +92-333-9478595 Date Submitted: September 15, 2021 Date Revised: July 06, 2023 Date Accepted: August 19, 2023 |
|
THIS ARTICLE MAY BE CITED AS: Saboor A, Khan MM, Afsar B, Khan AS. Serum E-Cadherin level in various clinical variants of oral potentially pre-malignant disorders. Khyber Med Univ J 2023;15(3):167-70. https://doi.org/10.35845/kmuj.2023.22813 |
ABSTRACT
OBJECTIVE: To compare the serum level of E-cadherin in clinical variants of oral potentially malignant disorders (OPMDs).
METHODS: This comparative cross-sectional study included eighty patients with OPMDs of Pakistani nationality, spanning all ages and both genders. Exclusion criteria encompassed cases that presented with squamous cell carcinoma and other non-OPMD pathologies. Age, gender, place of residence, lesion site, noxious habits, and habit duration were documented for all participants. The type of OPMDs was diagnosed by oral and maxillofacial surgeon and histopathologist. ELISA method was used for analysis of soluble E-cadherin levels in serum. Serum level of E-cadherin among various OPMDs were compared through One-way ANOVA.
RESULTS: Majority (n=64; 80%) of participants were using Snuff/Chewable tobacco and 12 (15%) were smokers. Leukoplakia (n=40; 50%) and Lichen Planus (n=28; 35%) were the common lesions and buccal mucosa (n=36; 45%) was the commonest site of lesion. Mean duration of lesion was 1.39±1.24 years. Mean E-cadherin was 26.34±3.67 ng/dl. The highest level of E-cadherin was found in carcinoma in-situ (32.0±2.33 ng/dl), oral submucous fibrosis (29.8±1.33 ng/dl) and Leukoplakia (26.7±3.11 ng/dl) and least in lichen planus (23.8±2.60 ng/dl) [p<0.001]. Post-hoc analysis showed statistically significant differences among various OPMDs (p<0.001) except between oral submucous fibrosis (OSF) and Leukoplakia (p=.108).
CONCLUSION: The expression of serum E-cadherin level is more in invasive OPMDs than less invasive OPMDs. These findings underscore the potential utility of E-cadherin as a biomarker for OPMD progression and prognosis. Further investigations are needed to explore the clinical implications and therapeutic relevance of these observed variations.
KEYWORDS: Cadherins (MeSH); E-Cadherin (MeSH); Oral premalignant disorder (Non-MeSH); Leukoplakia (MeSH); Oral Submucous Fibrosis (MeSH); Lichen Planus (MeSH).
INTRODUCTION
Oral premalignant disorders (OPMDs) are lesions which have the ability to transform into malignancy.1,2 The examples of OPMDs are carcinoma in situ, erythroplakia, leukoplakia, oral submucous fibrosis, actinic keratosis, oral lichen planus, tobacco pouch keratosis and palatal lesion of reverse cigar smoking.3 Multiple factors play role in rate of malignant transformation of these lesions like genetic, ethnic, gender of patient, behaviors and grade of dysplasia.4 Some rapid tests are always needed to predict the behaviors of these lesions and its associated morbidity and mortality.5 These premalignant lesions express various biomarkers which can predict the behavior and transformation of these OPMDs into oral squamous cell carcinoma (OSCC). Control of these biomarkers through therapeutic intervention can help arrest the progression of these disorders.6
Adhesion among cells in oral and in much extra oral tissue is accomplished by a specific protein called E-cadherin. This belongs to the family of cadherin proteins. The other types of cadherins are P-cadherin present in placenta, N-cadherin found in neuronal tissue, VE-cadherin present in vascular endothelium and R-cadherin found in retina.7
In case of OSCC because of unregulated growth the adhesion among cells is lost and level of E-cadherin increased in serum. So the serum level of E-cadherin can be used as biomarker to determine the invasiveness of oral lesions.8 Literature reported that upto 53.7 % cases with OSCC have increased serum E-cadherin level. It is suggested that serum E-cadherin level have diagnostic role in OSCC.9
Though plenty of literature is available on serum and saliva E-cadherin in patients with squamous cell carcinoma and other malignancies but there is lack of literature on serum level of E-cadherin in cases with orally potential malignant disorders (OPMDs). We wanted to probe whether a difference exist in expression of E-cadherin in various clinical variants of OPMDs. This study may reveal which OPMD is more aggressive and have more chance of malignancy. This study was planned to compare the serum level of E-cadherin in clinical variants of OPMDs.
METHODS
This cross sectional comparative study was conducted on 80 participants with OPMDs. Ethical approval was obtained from relevant institutes. The inclusion criteria were diagnosed cases by histopathology for OPMDs, Pakistani national, any age and both genders. Cases with squamous cell carcinoma and other pathologies than OPMDs were excluded. The collection of specimens was done at four dental and medical institutes of Khyber Pakhtunkhwa, Pakistan (Peshawar Medical College, Peshawar Dental College, Khyber College of Dentistry and Bacha Khan Dental College).
Patients who were already diagnosed with OPMD were interviewed to record age, gender, residence, site of lesion, noxious habits, and duration of habits. The type of OPMD was diagnosed by oral and maxillofacial surgeon and histopathologist. A verbal informed consent was taken from each participant after in-depth explanation of the study. Five milliliters of blood was collected from the participants ensuring aseptic technique. Centrifugation of the collected blood was performed at 4000rpm for 5 minutes to separate serum (HettichEBA 20 Germany). Serum aspiration was done through micropipettes followed by placement in serum cuvettes and storage at -20°Ċ till analysis. ELISA method was used for analysis for soluble E-cadherin levels in serum.
Analyses were done through R package (version 4.1.2). Frequency were computed for categorical data like gender, residence, education, habits, site, type of lesion (OPMDs) while mean and SD for numerical data like age of patients, duration of habits, duration of lesion , and E-cadherin level. One-way ANOVA was applied to compare E-cadherin among various OPMDs. Post hoc analysis was conducted using tukey test. Data were plotted graphically using box plot. For analyses the level of significance was P<0.05.
RESULTS
Out of 80 participants, 64 (80%) were males and 16 (20%) were females. The mean age of the participants was 53.05±14.50 years. Majority (n=58; 72%) were residing in rural areas and 54 (68%) participants were illiterate. Majority (n=50; 62%) were using Snuff/Chewable tobacco (smokeless tobacco) and 12 (15%) were smokers. The mean duration of habits was 18.85±14.27 years.
The most common sites of lesion were buccal mucosa (n=36; 45%) and lower ridge (n=10; 12%). Leukoplakia (n=40; 50%) and Lichen Planus (n=28; 35%) were the common lesions [Table I]. Mean Duration of lesion was 1.39±1.24 years.
Table I: Demographic and Clinical Characteristics of a Cohort with Oral
|
Parameter |
Characteristic |
Frequency (Percentage) (n=80) |
|
Gender |
Male |
64 (80) |
|
Female |
16 (20) |
|
|
Residence |
Rural |
58 (72) |
|
Urban |
22 (28) |
|
|
Education |
Graduate |
10 (12) |
|
Illiterate |
54 (68) |
|
|
Intermediate |
12 (15) |
|
|
Post grade |
4 (5.0) |
|
|
Habits |
Nil |
18 (22) |
|
Smoker |
12 (15) |
|
|
Snuff/Chewing tobacco |
50 (62) |
|
|
Site |
both Lower lip and alv ridge |
8 (10) |
|
Buccal mucosa |
36 (45) |
|
|
Gingiva |
4 (5.0) |
|
|
Lat. Tongue |
8 (10) |
|
|
lower lip |
6 (7.5) |
|
|
lower ridge |
10 (12) |
|
|
upper alv ridge |
8 (10) |
|
|
Lesion |
Carcinoma in situ |
7 (8.8) |
|
Leukoplakia |
40 (50) |
|
|
Lichen Planus |
28 (35) |
|
|
Oral submucous fibrosis |
5 (6.2) |
Mean E-cadherin was 26.34±3.67 ng/dl. The highest level of E-cadherin was found in carcinoma in-situ (32.0±2.33 ng/dl) followed by OSF (29.8±1.33 ng/dl). These differences for level of E-cadherin among OPMDs were very highly statistically significant (p<0.001). Post hoc analysis showed that the differences among various OPMDs were very highly statistically significant (p<0.001) except between OSF and leukoplakia (p=.108) (Table II).
Table II: Comparative Analysis of Differential E-cadherin Levels in Various Oral Potentially Malignant Disorders
|
Oral Potentially Malignant Disorders (OPMD) |
E-cadherin level (ng/dl) Mean (SD) |
P-value* |
Post hoc analysis (Tukey test) |
|
Carcinoma in situ (A) |
32.0 (2.33) |
<0.001 |
A vs B p<0.001 A vs D p<0.001 C vs D p<0.001 B vs C p=NS B vs D p<0.001 |
|
Oral submucous fibrosis (B) |
29.8 (1.33) |
||
|
Leukoplakia (C) |
26.7 (3.11) |
||
|
Lichen Planus (D) |
23.8 (2.60) |
*One way ANOVA tes
Figure 1 shows that carcinoma in situ have highest level of E-cadherin followed by OSF then leuloplakia and least Lichen Planus. The boxplots show only overlap between OSF and leukoplakia due to non-significant difference in E-cadherin level.
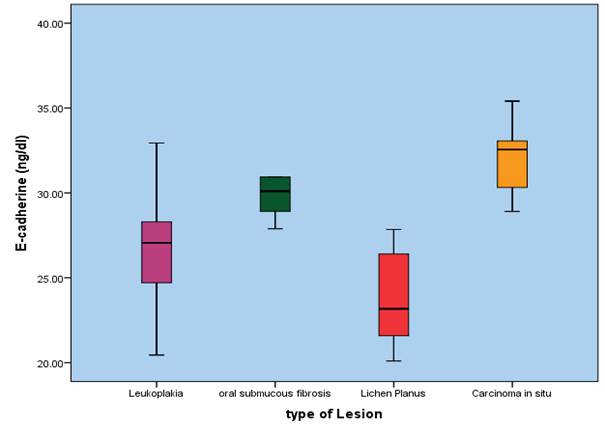
Figure 1: E-cadherin level among various Oral Potentially Malignant Disorders (OPMDs)
DISCUSSION
This investigation was aimed to compare the serum level of E-cadherin in clinical variants of oral potentially malignant disorders. Our findings showed that highest level of E-cadherin was found in carcinoma in-situ followed by OSF then leukoplakia and least in lichen planus. The difference was statistically significant.
Our findings showed that the males were 80%. This shows that OPMDs are higher in male gender in our population. The higher occurrence of OPMDs in males in our population can be attributed to higher frequency of noxcious habits in our males. Controversy exists in literature regarding the occurrence of OPMDs in males and females.10 A study conducted in India also reported that OPMDS are higher in males.11
Our finding shows that the most common site for OPMDs was buccal mucosa and most common premalignant lesion was leukoplakia followed by lichen planus. Previous study showed in 80% cases the oral lichen planus is present on buccal mucosa.12
E-cadherin can be located in a normal individual’s circulation (51.18–85.08 ng/ml)13 but high levels are observed in patients having malignancies. It is considered to be a very important prognostic marker in characterizing different carcinomas. However, its prognostic efficacy in identifying OPMDs is still not proven.14 The level of E-cadherin has been linked to the degree of invasiveness of carcinoma and other neoplastic lesions of breast. The more invasive the lesion the higher will be E-cadherin in serum.15
Our findings showed that highest level of E-cadherin was found in carcinoma in-situ followed by OSF then Leukoplakia and least in lichen planus. In case of pathology because of unregulated growth the adhesion among cells lost and level of E-cadherin increased in serum. So the serum level of E-cadherin can be used as biomarkers to determine the invasiveness of oral lesions.8
Our research is novel type of investigation comparing serum E-cadherin level in patient’s sera affected with OPMDs. The novelty of the present study can be best assessed from the fact that, to our knowledge, this is the first study conducted on the serum samples of OPMDs patients for the assessment of soluble E-cadherin levels. There are two studies conducted on the E-cadherin levels in the salivary samples of OSCC and serum of head and neck squamous cell carcinoma (HNSCC) patients.16 Al Kassam et al., found high serum levels of soluble E-cadherin among 39 cases of HNSCC, to be significantly different from those in the control group, comprising of 10 subjects.16 Lopez-Verdin et al., found increase in salivary E-cadherin levels among 26 cases of OSCC compared to 10 individuals without oral carcinoma.17
CONCLUSION
Within the limitations of this study it can be concluded that the expression of serum E-cadherin level is more in invasive OPMDs than less invasive OPMDs. Serum E-cadherin can be used as biomarker or prognosis of OPMDs.
REFERENCES
1. Ray JG. Oral potentially malignant disorders: Revisited. J Oral Maxillofac Pathol 2017;21(3):326-7. https://doi.org/10.4103/jomfp.JOMFP_224_17
2. Amagasa T, Yamashiro M, Uzawa N. Oral premalignant lesions: from a clinical perspective. Int J Clini Oncol 2011;16(1):5-14. https://doi.org/10.1007/s10147-010-0157-3
3. Mortazavi H, Baharvand M, Mehdipour M. Oral potentially malignant disorders: an overview of more than 20 entities. J Dent Res Dent Clin Dent Prospects 2014;8(1):6. https://doi.org/10.5681/joddd.2014.002
4. Speight PM, Khurram SA, Kujan O. Oral potentially malignant disorders: risk of progression to malignancy. J Dent Res Dent Clin Dent Prospects 2018;125(6):612-27. https://doi.org/10.1016/j.oooo.2017.12.011
5. Ganly I, Patel S, Shah J. Early stage squamous cell cancer of the oral tongue—clinicopathologic features affecting outcome. Cancer 2012;118(1):101-11. https://doi.org/10.1002/cncr.26229
6. Carmeliet P, Jain RK. Molecular mechanisms and clinical applications of angiogenesis. Nature 2011;473(7347):298-307. https://doi.org/10.1038/nature10144
7.Orsenigo F, Giampietro C, Ferrari A, Corada M, Galaup A, Sigismund S, et al. Phosphorylation of VE-cadherin is modulated by haemodynamic forces and contributes to the regulation of vascular permeability in vivo. Nature Commun 2012;3(1):1-15. https://doi.org/10.1038/ncomms2199
8. Hashimoto T, Soeno Y, Maeda G, Taya Y, Aoba T, Nasu M, et al. Progression of oral squamous cell carcinoma accompanied with reduced E-cadherin expression but not cadherin switch. PLoS One 2012;7(1):e47899. https://doi.org/10.1371/journal.pone.0047899
9. Hazan RB, Qiao R, Keren R, Badano I, Suyama K. Cadherin switch in tumor progression. Ann N Y Acad Sci 2004;1014(1):155-63. https://doi.org/10.1196/annals.1294.016
10. Yardimci G, Kutlubay Z, Engin B, Tuzun Y. Precancerous lesions of oral mucosa. World J Clin Cases 2014;2(12):866. https://doi.org/10.12998/wjcc.v2.i12.866
11. Srivastava R, Sharma L, Pradhan D, Jyoti B, Singh O. Prevalence of oral premalignant lesions and conditions among the population of Kanpur City, India: A cross-sectional study. J Fam Med Primary Care 2020;9(2):1080-5. https://doi.org/10.4103/jfmpc.jfmpc_912_19
12. Dissemond J. Oral lichen planus: an overview. J Dermatological Treat 2004;15(3):136-40. https://doi.org/10.4103/0975-7406.155873
13. Cepowicz D, Zaręba K, Pryczynicz A, Dawidziuk T, Żurawska J, Hołody-Zaręba J, et al. Blood serum levels of E-cadherin in patients with colorectal cancer. Gastroenterol Rev 2017;12(3):186-91. https://doi.org/10.5114/pg.2017.70471
14. Zuo JH, Zhu W, Li MY, Li XH, Yi H, Zeng GQ, et al. Activation of EGFR promotes squamous carcinoma SCC10A cell migration and invasion via inducing EMT‐like phenotype change and MMP‐9‐mediated degradation of E‐cadherin. J Cell Biochem 2011;112(9):2508-17. https://doi.org/10.1002/jcb.23175
15. Pai K, Baliga P, Shrestha BL. E-cadherin expression: a diagnostic utility for differentiating breast carcinomas with ductal and lobular morphologies. J Clin Diagn Res 2013;7(5):840-4. https://doi.org/10.7860/JCDR/2013/5755.2954
16. Al Kassam D, Blanco I, de Los Toyos J, Llorente J. Diagnostic value of E-cadherin, MMP-9, activated MMP-13 and anti-p53 antibodies in squamous cell carcinomas of head and neck. Med Clin 2007;129(20):761-5. https://doi.org/10.1157/13113764
17. López-Verdín S, de la Luz Martínez-Fierro M, Garza-Veloz I, Zamora-Perez A, Grajeda-Cruz J, González-González R, et al. E-Cadherin gene expression in oral cancer: Clinical and prospective data. Med Oral Patologia Oral Cirugia Bucal 2019;24(4):e444. https://doi.org/10.4317/medoral.23029
|
Following authors have made substantial contributions to the manuscript as under:
AS: Concept and study design, acquisition of data, drafting the manuscript, approval of the final version to be published MMK: Concept and study design, analysis and interpretation of data, critical review, approval of the final version to be published BA & ASK: Analysis and interpretation of data, drafting the manuscript, critical review, approval of the final version to be published Authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST Authors declared no conflict of interest
GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |