![]() https://doi.org/10.35845/kmuj.2023.22653 ORIGINAL
ARTICLE
https://doi.org/10.35845/kmuj.2023.22653 ORIGINAL
ARTICLE
Anxiety, depression and low self-esteem among people with alopecia
Gati
Ara 1,2 ![]() ,
Waqar Tunio 3, Noor Imran Khan 4, Abeel Tariq 4,
Tamjeed Jamshed 4
,
Waqar Tunio 3, Noor Imran Khan 4, Abeel Tariq 4,
Tamjeed Jamshed 4
|
1: Department of Community Medicine, Dow Medical College, Dow University of Health Sciences, Karachi, Pakistan 2: Department of Community Health Sciences, Ziauddin University, Karachi, Pakistan 3: Resident Medical Officer, Plastic Surgery, Laser Inn Aesthetic Surgery Center, Karachi, Pakistan 4: Final year MBBS, Ziauddin University, Karachi, Pakistan
Email
Contact #: +92-321-2117446 Date Submitted: March 24, 2022 Date Revised: September 05, 2023 Date Accepted: September 15, 2023 |
|
THIS ARTICLE MAY BE CITED AS: Ara G, Tunio W, Khan NI, Tariq A, Jamshed T. Anxiety, depression and low self-esteem among people with alopecia. Khyber Med Univ J 2023;15(3):161-6. https://doi.org/10.35845/kmuj.2023.22653 |
ABSTRACT
OBJECTIVES: To assess the frequency of anxiety and depression symptoms among individuals with alopecia and to assess the self-esteem levels of alopecia patients in a hair restorative treatment center of Karachi, Pakistan.
METHODS: This cross-sectional study was conducted on 84 consecutive patients of Alopecia by conducting interviews. Sample size was calculated using the prevalence rate of alopecia of 2% at confidence level of 95% and precision of 3%. Hospital Anxiety and Depression Scale (HADS) which was used to quantify depression and anxiety, and Rosenberg Self-esteem Scale (RSES) was used for self- esteem levels. Scores were calculated. Test of correlation and Chi square test were applied.
RESULTS: Median (inter-quartile range) HADS score for Anxiety and Depression in 84 study participants was 11 (7-14) and 11 (8-14) respectively. Regarding depression and depression, 52.4% (n=44) and 53.6% (n=45) fell into the abnormal category (score 11-21) respectively. For self-esteem, 48.8% (n=41) had low self-esteem (score 0-14). Positive correlation was found between age of participants and their self- esteem score (p- value =0.001). The older participants achieved higher scores. There was an inverse relation between age at onset of alopecia and self-esteem score (p-value= 0.03). People with early onset of Alopecia had lower self-esteem scores. There was no significant difference between male and females and the anxiety, depression and self-esteem levels.
CONCLUSION: Our study reveals significant prevalence of depression, anxiety, and low self-esteem among alopecia patients seeking hair restoration, highlighting the urgent need for targeted psychological interventions.
KEY WORDS: Alopecia (MeSH); Alopecia Areata (MeSH); Hair (MeSH); Depression (MeSH); Anxiety (MeSH); Self-esteem (Non-MeSH); Hospital Anxiety and Depression Scale (Non-MeSH); HADS (Non-MeSH); Rosenberg Self- Esteem Scale (Non-MeSH); RSES (Non-MeSH).
INTRODUCTION
Alopecia is a skin disorder resulting in hair loss (baldness).1 It is a skin disorder that distresses both genders of all ages.2 The etiopathogenesis of alopecia includes genetic factors, various infections, psychological factors, autoimmune diseases and chemotherapy.2 Alopecia areata (AA) is a scalp or body hair loss condition that affects up to 2% of the population. It is an inflammatory scalp due to autoimmune response. It leads to non-scarring scalp with patchy hair loss that may affect the full scalp causing Alopecia Totalis or cause loss of all body hair leading to Alopecia Universalis.3,4 The prevalence of Alopecia Aerata differs by region and is increasing over time.4
In Androgenic Alopecia known as male-pattern baldness, the hair is lost in a well-defined pattern resulting in a hairline of typical “M” shape. Some individuals’ hair also becomes thin and sparse at the crown that often progresses to complete baldness.5 Traction Alopecia is hair loss induced due to constant drawing (traction) of hair because of tight hairstyles.6 Trichotillomania is a different condition where individuals have active desire to pull their own hair.6
Alopecia is not a lethal condition but it can have an enormous influence on self-perception and quality of life.7 Some past studies have testified that alopecia areata disturbs the quality of life.8 This is especially true for women with alopecia, who have been shown to experience poorer psychological outcomes compared with men.8 Hair represents an essential element of attractiveness and femininity for females in most cultures.9 Most physicians focus only on the diagnosis and management of the disease and fail to realize some of the psychosocial issues that may arise due to hair loss.10
Alopecia can lead to a chronic nature of mental disturbances regarding self-image due to the lack of hope of complete and speedy recovery from the disease. A study in Iran found an association of Alopecia with anxiety (OR= 2.72) and depression (OR=4.48) 11 Chu et al found that people with alopecia Areata tend to have higher coexisting Anxiety.12 An imperative phenomenal analysis of adolescents in Pakistan’s Punjab province found loss of self- esteem in females and self confidence in both males and female adolescents living with Alopecia Areata.13
A study by Marahatta S, et al found the prevalence of depression among Alopecia Areata patients to be 66.7% with moderate to severe depression in about 18%.14 Identification of the adverse psychological effects of alopecia like depression and low self -esteem is necessary. Past studies indicate the psychological effects on Alopecia patients especially depression. Most research into the psychological problems relating to alopecia has been part of another aim such as effects of a treatment. No quantitative study is available in Pakistan that assesses the association of Alopecia with anxiety and depression. And no thorough study has been conducted to estimate the self- esteem of people living with Alopecia. This study aims to estimate anxiety, depression and low self-esteem in patients with alopecia.
METHODS
This cross-sectional study was conducted amongst individuals diagnosed with alopecia in a hair restorative clinic in Karachi. A sample size of 84 was calculated from openepi.com sample size calculator using the prevalence rate of alopecia of 2% at confidence level of 95% and precision of 3%. Individuals of both genders, with all types of Alopecia over the age of 18 years were selected through consecutive sampling technique. Individuals with undiagnosed alopecia or chemotherapy patients were excluded from the study.
Data was collected using Consecutive sampling technique via interviewing participants. Diagnosis of alopecia was made by certified medical practitioner at the clinic as “visible appearance of hair loss or receding hairline”.5 Once the diagnosis was established by the certified practitioner, research investigators enrolled participants and asked detailed history regarding age of onset, duration of disease and its associated symptoms. Thereafter, to quantify depression and anxiety, HADS (Hospital Anxiety and Depression Scale) was used and for quantification of self-esteem the Rosenberg Self-esteem Scale was used. HADS is a valid and reliable tool to assess patients for anxiety and depression in the medical out-patient setting.15 Total 14 questions are asked, 7 for assessment of anxiety and 7 for estimation of depression. The score of each question ranges from 0 to 4. Thus, minimum score of zero to maximum score of 21 is attainable for both anxiety and depression separately. The classification divides respondents into three categories: Normal Score= 0-7, borderline abnormal (borderline case) = 8-10, Abnormal (Case) = 11-21.15 For the assessment of Self- esteem Rosenberg Self-esteem Scale was used. Rosenberg self-esteem scale is a unidimensional scale. All items are answered using a 4point Likert scale format ranging from strongly agree to strongly disagree. The responses carry a score of 0 to 3. There are total 10 questions with a total score of minimum 0 to maximum 30. Scores below 15 represent problematic low self-esteem.16
Approval for the research was taken for Ziauddin University. Permission for data collection was taken from laser in hair restoration clinic. Prior written informed consent was taken from each participant. Anonymity was maintained and data was kept confidential. Data was used for academic purpose only. No monetary benefits were provided to the participants.
Data was analyzed using SPSS 20. Quantitative variables were such as age, scores were represented as mean and standard deviation. Qualitative variables such as marital status, education, profession and co-morbid conditions were denoted as frequency and percentage. Mean scores were calculated for anxiety and depression. The scores were then categorized according to HADS classification of normal (0-7), borderline (8-10) and abnormal case (11-21). Mean score for self- esteem was calculated according to Rosenberg self-esteem scale. The scores were later categorized as low self- esteem (0-14) and normal to high self- esteem (15-30). Test of correlation was applied for finding correlation between dependent and independent variables. Chi square was applied to compare the depression, anxiety and self-esteem scores with respect to gender, age, and age at onset of Alopecia. P- value of less than 0.03 was taken as significant.
RESULTS
A sample size of 84 with mean age of 43.15±14 years with majority falling in their 30s was selected for the study. The sociodemographic characteristics of participants are given in Table I.
Table I: Sociodemographic characteristics of the participants
|
Variable |
Frequency (n=84) |
Percentage |
|
|
Gender |
Male |
75 |
89.3 |
|
Female |
9 |
10.7 |
|
|
Marital status |
Single |
24 |
28.6 |
|
Married |
44 |
52.4 |
|
|
Divorced |
12 |
14.3 |
|
|
Widow/widower |
4 |
4.7 |
|
|
Educational status |
Graduates |
60 |
71.4 |
|
Intermediate/ A level IGCSE |
4 |
4.7 |
|
|
Undergraduate students |
18 |
21.4 |
|
|
Other |
2 |
2.4 |
|
|
Profession |
Banking and Accountants |
17 |
20.2 |
|
Teaching |
10 |
11.9 |
|
|
Sales and Marketing |
8 |
9.5 |
|
|
Doctor |
7 |
8.3 |
|
|
Lawyer |
7 |
8.3 |
|
|
Business and management |
6 |
7.1 |
|
|
Student |
6 |
7.1 |
|
|
Engineering and IT |
5 |
6 |
|
|
Housewife |
3 |
3.6 |
|
|
Architect |
2 |
2.3 |
|
|
Acting |
1 |
1.2 |
|
|
Chef |
1 |
1.2 |
|
|
Yoga instructor |
1 |
1.2 |
|
|
Others |
10 |
11.9 |
|
IGCSE: International General Certificate of Secondary education
Majority (n=44; 52.4%) of participants had co-morbid conditions. Hypertension was the most frequent (n=37; 44.1%) followed by diabetes (n=16; 19%). Most (n=49; 58.3%) participants were taking different medications. Antihypertensives were being taken by 24 (28.6%) and Finasteride by 23 (27.4%) participants.
Family history of alopecia was positive among 57 (67.9%) participants. Mean age of Alopecia onset was 29±9 years. Most (n=61; 72.6%) of the participants were unaware of the degree of their alopecia
Median (inter-quartile range) HADS score for Anxiety and Depression in 84 study participants was 11 (7-14) and 11 (8-14) respectively. Median self-esteem score of the participants was 15 (IQR=11-21) out of the maximum attainable score of 30. Most frequently attained score (mode) was 12. The scores were categorized into low self- esteem score (0-14) and normal score (15 and above). Regarding depression and depression, 52.4% and 53.6% fell into the abnormal category (score 11-21) respectively. For self-esteem, 48.8% had low self-esteem (score 0-14), while 51.2% fell into the normal to high self-esteem category (15-30) [Table II].
Table II: Psychological Well-being Assessment: Depression, Anxiety, and Self-esteem Scores among Participants
|
Variables |
Score# |
Frequency (n=84) |
Percentage (%) |
|
|
Status of Depression |
Normal |
0-7 |
16 |
19 |
|
Borderline Case |
8-10 |
15 |
17.9 |
|
|
Abnormal Case |
11-21 |
44 |
52.4 |
|
|
Status of Anxiety |
Normal |
0-7 |
25 |
29.8 |
|
Borderline Case |
8-10 |
12 |
14.3 |
|
|
Abnormal Case |
11-21 |
45 |
53.6 |
|
|
Self Esteem Level |
Low self esteem |
0-14 |
41 |
48.8 |
|
Normal to high self esteem |
15-30 |
43 |
51.2 |
|
#Hospital Anxiety and Depression Scale for depression & Anxiety & Rosenberg score for Self- esteem
Positive correlation was found between age of participants and their self- esteem score (p- value =0.001). The older participants achieved higher self-esteem scores.
Correlation of Age at onset of Alopecia with anxiety and Depression scores are given in figure 1 and figure 2 respectively.
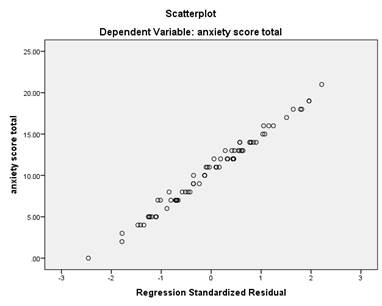
Figure I: Age at onset of Alopecia and Anxiety score (R square= 0.008, p value=0.419)
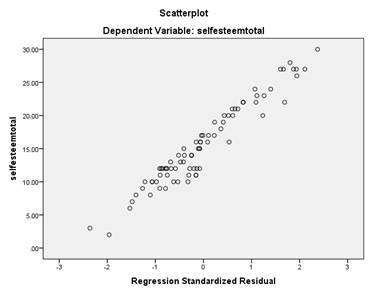
Figure 2: Age at onset of Alopecia and Depression score (R square=0.104, p value= 0.005)
There was a significant inverse liner relation between age at onset of alopecia and self-esteem (p-value= 0.02). People with early onset of Alopecia had lower self-esteem scores. Figure 3.
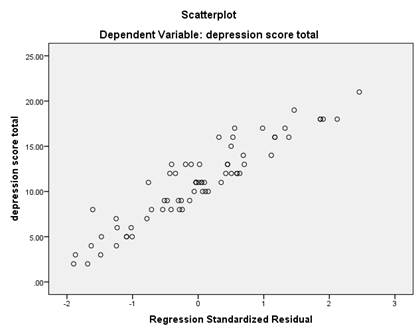
Figure 3: Age at onset of Alopecia and Self- esteem score. (R square=0.066, p value =0.02)
There was no significant difference between male and females and the anxiety, depression and self-esteem categories.
The age of participants and age at onset of Alopecia were not found to be associated with anxiety, depression and self-esteem levels.
DISCUSSION
The study has yielded interesting results. It must be noted that self-assessment tools are for screening purposes and definitive diagnosis is dependent on clinical examination by trained practitioner. 17 HADS is a simple yet reliable tool for use in hospital setting, primary care or even community. 17
Most participants in this study were found to have an abnormal case of depression n=44 (52%) while 15 (18%) were borderline. This is an enormously high frequency even when compared to the staggering prevalence of depression in the general population of Karachi which is 34%.18 An analogous prevalence of depression was established in a research in Iran by Baghestani et al.11 However, an even higher frequency of depression was reported in a study on 75 patients done by Marahatta et al who estimated the prevalence of depression to be whopping 66.7% among Alopecia patients.14 An earlier study by Mahsa et al found the prevalence of mild, moderate and severe depression to be 30, 22 and 9 percent respectively.8 Our results are also comparable to 50% major depression in Alopecia patients as reported by Gokalp.19
Most participants in our study were hypertensive but our estimated prevalence is much higher that the reported prevalence of depression in the hypertensive population that is 21.3% 19
The reported prevalence of anxiety in population of Karachi is 27.4%. 20The frequency of anxiety in our participants was n=45 (54%) cases and n=12 (14%) the borderline cases. This is much higher than the reported prevalence for general population as well as people with rare chronic diseases. 21. However, it is lower than that reported by Chikere Ifeanyi C et al among hypertensive patients.in Nigeria. 22
This study found an alarming low self-esteem frequency of 41 (49%) among the people living with Alopecia. Previously, very few studies have quantitatively assessed self-esteem levels of Alopecia patients. Past study on Androgenic alopecia patients concluded that hair transplant significantly boosts self-esteem levels.23 A 2020 study by Askin et al used the same Rosenberg scale as this study for assessment of self-esteem in 64 children and adolescents.24 They discovered that the proportion of cases of Alopecia with moderate and low self-esteem scores was significantly higher in Cases of Alopecia as compared to the controls (p=0.001).24 They concluded that hair loss is a significant factor affecting self-esteem. 24
Alopecia has been shown to cause higher rates of anxiety and depression in children, adolescents and women. 25 Traditionally, alopecia was considered an aesthetic concern only, however it comprises a momentous burden of psychosocial insinuations, and thus should be evaluated within a proper medical model.9
CONCLUSION
Our study underscores a substantial occurrence of depression, anxiety, and low self-esteem among alopecia patients seeking hair restoration, underscoring the critical need for targeted psychological interventions. Compared to general population rates and those with chronic diseases, alopecia patients exhibit heightened frequencies of anxiety and depression, with nearly half experiencing low self-esteem. This emphasizes the importance of routine examinations for psychological comorbidities in alopecia patients to enable timely, effective, and holistic interventions, ultimately enhancing their overall quality of life. Additionally, we recommend further research involving pre and post hair restoration assessments for anxiety and depression.
ACKNOWLEDGEMENTS
We are grateful to Dr. Zulfiqar H. Tunio for the kind permission of data Collection from his hair restoration center.
REFERENCES
1. Anon. Alopecia. [internet] The Free Dictionary. 2012 [Accessed on: February 15, 2023]. Available from URL: https://medical-dictionary.thefreedictionary.com/alopecia
2. Gokalp H. Psychosocial Aspects of Hair Loss [Internet]. Hair and Scalp Disorders. InTech; 2017 [Accessed on: February 15, 2023]. Available from URL: http://dx.doi.org/10.5772/66156
3. Singh K, Saeed F, Ahmad Z, Ahsan F, Shakya P. Alopecia: introduction and overview of herbal treatment. J Chem Pharm Res 2016;8(8):59-64.
4. Lee HH, Gwillim E, Patel KR, Hua T, Rastogi S, Ibler E et al. Epidemiology of alopecia areata, ophiasis, totalis, and universalis: A systematic review and meta-analysis. J Am Acad Dermatol 2020;82(3):675-82. https://doi.org/10.1016/j.jaad.2019.08.032
5. Amoretti A, Laydner H, Bergfeld W. Androgenetic alopecia and risk of prostate cancer: a systematic review and meta-analysis. J Am Acad Dermatol 2013;68(6):937-43. https://doi.org/10.1016/J.JAAD.2012.11.034
6. Foundation BS. Traction alopecia. [Internet]. British Skin Foundation. 2022 [Accessed on: February 15, 2023]. Available from URL: https://knowyourskin.britishskinfoundation.org.uk/condition/traction-alopecia/
7. Pradhan P, D’Souza M, Bade BA, Thappa DM, Chandrashekar L. Psychosocial impact of cicatricial alopecias. Indian J Dermatol 2011;56(6):684. https://doi.org/10.4103/0019-5154.91829
8. Ghajarzadeh M, Ghiasi M, Kheirkhah S. Depression and quality of life in Iranian patients with Alopecia Areata. Iran J Dermatol 2011;14(4):140-3.
9. Marks DH, Penzi LR, Ibler E, Manatis-LA, Hagigeorges D, Yasuda M et al. The medical and psychosocial associations of alopecia: recognizing hair loss as more than a cosmetic concern. Am J Clin Dermatol 2019;20:195-200. https://doi.org/10.1007/S40257-018-0405-2
10. Hunt N, McHale S. Reported experiences of persons with alopecia areata. J Loss Trauma 2004;10(1):33-50. https://doi.org/10.1080/15325020490890633
11. Baghestani S, Zare S, Seddigh SH. Severity of depression and anxiety in patients with alopecia areata in Bandar Abbas, Iran. Dermatol Reports 2015;7(3). https://doi.org/10.4081/DR.2015.6063
12. Chu SY, Chen YJ, Tseng WC, Lin MW, Chen TJ, Hwang CY et al. Psychiatric comorbidities in patients with alopecia areata in Taiwan: a case–control study. Br J Dermatol 2012;166(3):525-31. https://doi.org/10.1111/J.1365-2133.2011.10714.X
13. Rafique R, Hunt N. Experiences and coping behaviours of adolescents in Pakistan with alopecia areata: An interpretative phenomenological analysis. Int J Qual Stud Health Well-being 2015;10(1):26039. https://doi.org/10.3402/QHW.V10.26039
14. Marahatta S, Agrawal S, Adhikari BR. Psychological impact of alopecia areata. Dermatol Res Pract 2020;2020:8879343. https://doi.org/10.1155/2020/8879343
15. Billy. The Hospital Anxiety and Depression Scale [Internet]. Dreams to Realities. 2018 [Accessed on: February 15, 2023]. Available from URL: http://dreamstorealities.co.uk/hads-self-test-questionnaire/
16. Rosenberg M. Rosenberg Self Esteem Scale [Internet]. American Psychological Association. [Accessed on: February 15, 2023]. Available from URL: https://www.apa.org/obesity-guideline/rosenberg-self-esteem.pdf
17. Snaith RP. The hospital anxiety and depression scale. Health and quality of life outcomes. 2003;1(1):1-4. https://doi.org/10.1186/1477-7525-1-29
18. Mansoor H. “Depression rising alarmingly in Pakistan’s urban areas” [Internet]. DAWN.COM. 2017 [Accessed on: February 15, 2023]. Available from URL: https://www.dawn.com/news/1325360
19. Godil A, Mallick MS, Adam AM, Haq A, Khetpal A, Afzal R, et al. Prevalence and severity of depression in a Pakistani population with at least one major chronic disease. J Clin Diagnostic Res 2017;11(8):OC05. https://doi.org/10.7860/JCDR/2017/27519.10329
20. F Farooq S, Khan T, Zaheer S, Shafique K. Prevalence of anxiety and depressive symptoms and their association with multimorbidity and demographic factors: a community-based, cross-sectional survey in Karachi, Pakistan. BMJ Open 2019;9(11):e029315. https://doi.org/10.1136/BMJOPEN-2019-029315
21. Uhlenbusch N, Löwe B, Härter M, Schramm C, Weiler-Normann C, Depping MK. Depression and anxiety in patients with different rare chronic diseases: A cross-sectional study. PLoS One 2019;14(2):e0211343. https://doi.org/10.1371/JOURNAL.PONE.0211343
22. Chikere IC, Ugonma WD, Somtochukwu MO, Angela JO, Uchenna LI, Queen K, et al. Prevalence of perceived depression and anxiety among hypertensives attending imo specialist hospital Owerri, Nigeria. Arch Depress Anxiety 2020;45-9. https://doi.org/10.17352/2455-5460.000051
23. Liu F, Miao Y, Li X, Qu Q, Liu Y, Li K, et al. The relationship between self‐esteem and hair transplantation satisfaction in male androgenetic alopecia patients. J Cosmet Dermatol 2019;18(5):1441-7. https://doi.org/10.1111/JOCD.12839
24. Aşkın Ö, Koyuncu Z, Serdaroğlu S. Association of alopecia with self-esteem in children and adolescents. Int J Adolesc Med Health 2020;34(5):315-8. https://doi.org/10.1515/IJAMH-2020-0100
25. Teichgräber F, Jacob L, Koyanagi A, Shin JI, Seiringer P, Kostev K. Association between skin disorders and depression in children and adolescents: A retrospective case-control study. J Affect Disord 2021;282:939-44. https://doi.org/10.1016/J.JAD.2021.01.002
|
Following authors have made substantial contributions to the manuscript as under: GA: Conception and study design, analysis and interpretation of data, drafting the manuscript, critical review, approval of the final version to be published. WT & NIK: Conception and Study Design, acquisition of data, critical review, approval of the final version to be published. AT, TJ: Acquisition of data, drafting the manuscript, approval of the final version to be published Authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. |
|
CONFLICT OF INTEREST Authors declared no conflict of interest GRANT SUPPORT AND FINANCIAL DISCLOSURE Authors declared no specific grant for this research from any funding agency in the public, commercial or non-profit sectors |
|
DATA SHARING STATEMENT The data that support the findings of this study are available from the corresponding author upon reasonable request |
|
|
|
KMUJ web address: www.kmuj.kmu.edu.pk Email address: kmuj@kmu.edu.pk |